

The First Five Years of Clinical Practice: Why Therapists Burn Out Early
There’s a Story We Don’t Tell Clearly Enough
SB Webb Counseling & Consulting PLLC | The Practice Library™
sbwebbcounselingconsulting.org
Before a clinician ever reaches their first session, there has already been an enormous lift.
Graduate school is not neutral. It requires time, money, unpaid labor, emotional investment, and often significant personal sacrifice. Many clinicians move through programs while working, parenting, caregiving, or navigating their own healing.
By the time someone graduates, they are not just “new.” They are often already stretched thin.
And yet, graduation is where the real pressure begins.
“We prepare clinicians to begin—but not always to sustain.”
The Gap Between Training and Reality
Clinical training teaches theory, ethics, and foundational skills. What it often does not fully prepare clinicians for is:
High acuity caseloads
Productivity expectations
Documentation tied to medical necessity
Insurance-driven care models
Isolation in practice settings
New clinicians step into systems that expect competence, efficiency, and emotional endurance—often immediately.
This gap is where burnout begins to take root.
The First Five Years: A High-Risk Window
The period between associate licensure and full licensure is one of the most vulnerable phases in a clinician’s career.
It is also where we lose a significant portion of the workforce.
Estimates have suggested that a large percentage of clinicians do not make it through to full licensure—often cited as more than half in some discussions of workforce retention. While exact figures vary by discipline and region, the pattern is consistent:
We are losing clinicians during the exact phase we should be developing them.
This is not simply an individual problem. It is a systems issue.
“The first five years are not just a training period—they are a retention crisis.”
The Reality of Early Clinical Work
Early career clinicians are often navigating:
High emotional labor without consistent containment
Complex client presentations
Pressure to "get it right"
Documentation expectations that directly impact reimbursement
Limited control over caseload composition
At the same time, many are trying to build confidence, develop clinical judgment, and understand how to translate theory into practice.
This is not a simple learning curve—it is a convergence of demands.
Developmental Stages of a Therapist
This developmental process does not happen in isolation. It is supported—and sometimes hindered—by how clinicians are trained to think, document, and engage in supervision.
Across clinical work, three interconnected systems shape development:
Clinical thinking and documentation
Developmental stage progression
The supervision ecosystem
When these systems are aligned, clinicians grow. When they are fragmented, burnout accelerates.
The Clinical Thinking & Documentation Loop
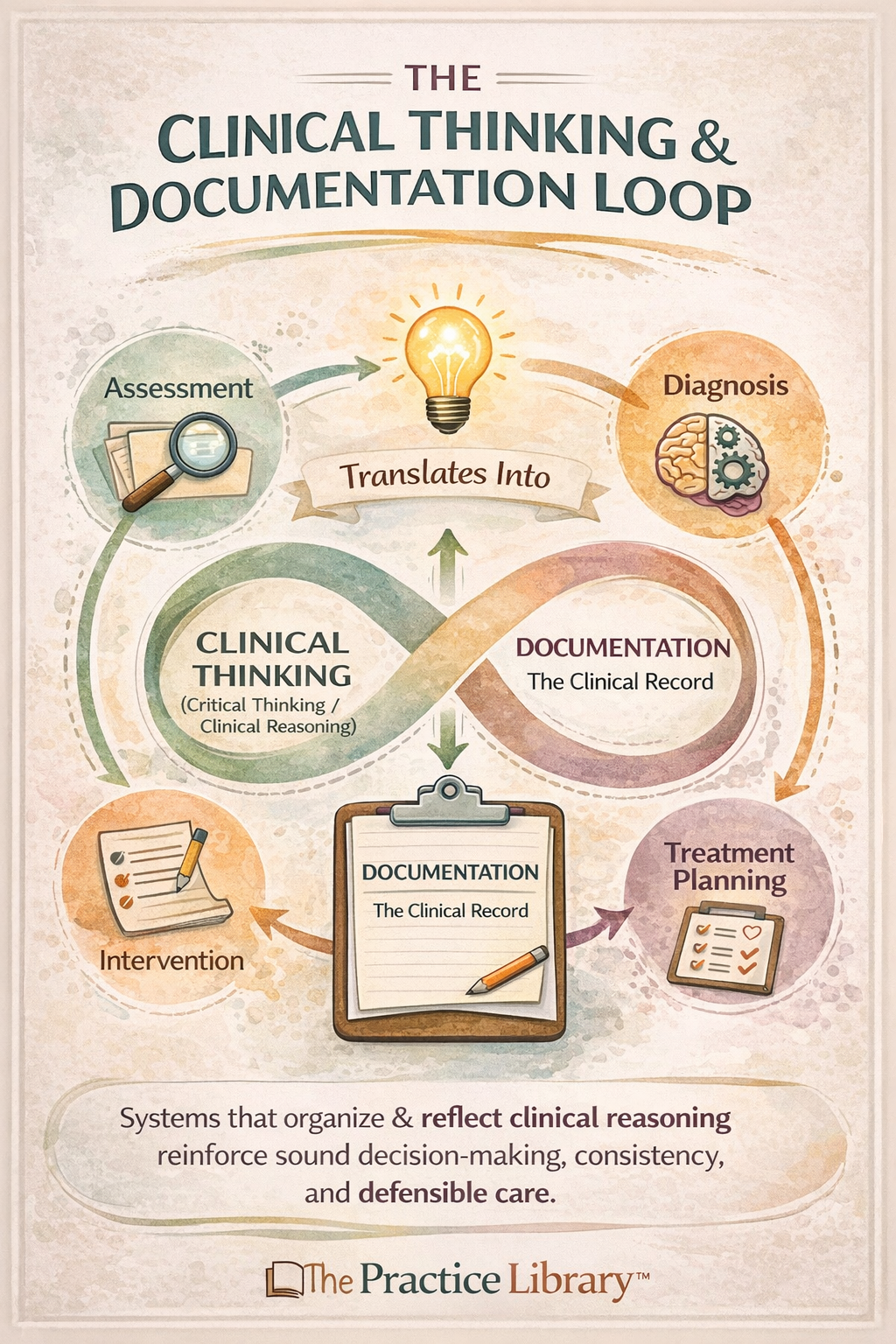
Clinical thinking is not separate from documentation—it is made visible through it.
Early clinicians are not just learning how to provide therapy—they are learning how to think clinically and translate that thinking into documentation that meets medical necessity and compliance standards.
This creates a continuous loop:
Assessment informs clinical thinking
Clinical thinking informs diagnosis and treatment planning
Treatment planning guides intervention
Intervention must be documented clearly and defensibly
Documentation reinforces (or challenges) clinical reasoning
When clinicians are not trained in this loop, documentation becomes overwhelming—and disconnected from clinical identity.
“Documentation is not separate from clinical work—it is clinical thinking made visible”
This process is often under-taught in early clinical training, which can leave clinicians feeling overwhelmed and disconnected from their own clinical reasoning. For a deeper breakdown of how documentation reflects clinical thinking and medical necessity, see my articles on medical necessity documentation, diagnostic formulation, and the golden thread in clinical care.
The Supervision Ecosystem
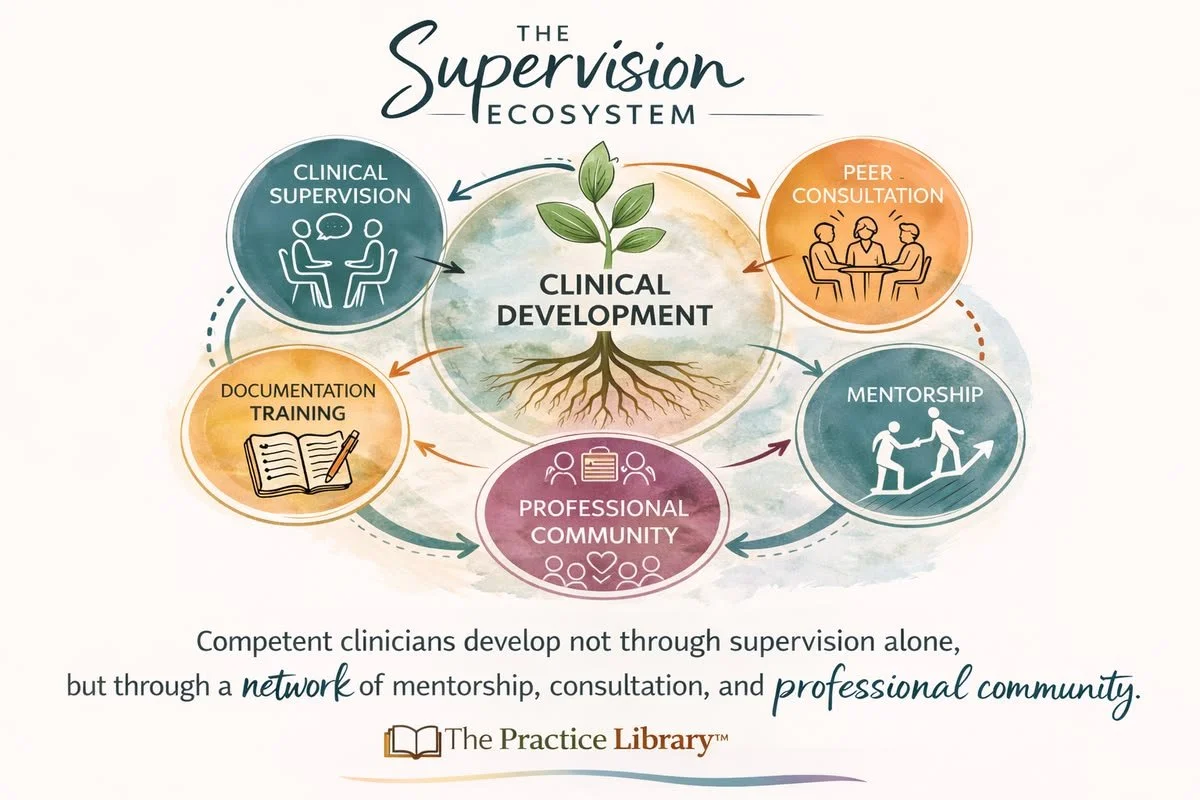
Clinical growth occurs within a broader ecosystem—not supervision alone.
Supervision alone is not enough to support development.
Clinicians grow within a broader ecosystem that includes:
Clinical supervision
Peer consultation
Mentorship
Documentation training
Professional community
When one or more of these elements are missing, clinicians often experience:
Increased isolation
Reduced confidence
Slower development of clinical judgment
“Supervision is not a requirement—it is a developmental lifeline”
This is especially critical in the first five years, when clinicians are forming their professional identity.
This broader framework is explored more fully in my work on the Supervision Ecosystem Model, which outlines how clinicians develop through interconnected systems of supervision, consultation, mentorship, and professional community.
The Supervisor Development Lens
An often-overlooked variable in early clinician burnout is not just whether supervision is occurring—but how developed the supervisor is in their role.
Supervisors, like clinicians, move through developmental stages. These can include roles such as:
Teacher (structure, skills, direction)
Guide (mentorship, reflection, integration)
Gatekeeper (standards, ethics, accountability)
Consultant (collegial dialogue, advanced clinical thinking)
When there is a mismatch between what a developing clinician needs and how a supervisor is practicing, tension can emerge.
For example, rigidity in supervision may reflect:
A supervisor primarily operating from a gatekeeping or early-stage teaching stance
Limited flexibility in adapting to a clinician’s developmental stage
A system emphasizing compliance over growth
For new clinicians, this creates an important reflective question:
“At what stage is my supervisor in their development—and how is that shaping the supervision I’m receiving?”
This becomes particularly important when considering the responsibility of supervision itself, which extends beyond oversight into the active development of another clinician’s professional identity. I explore these concepts further in past articles, including Uplift the Workforce: Why Supervision Is More Than Oversight and Becoming an Approved Supervisor in Washington: Beyond the 25-Hour Requirement.
This question is not about criticism. It is about understanding the supervisory dynamic as part of the broader developmental system.
“Not all supervision develops clinicians—and not all supervisors are at the same stage of development.”
When supervision evolves alongside the clinician, it becomes a powerful protective factor against burnout.
When it remains rigid or misaligned, it can unintentionally contribute to it.
Developmental Stages of a Therapist
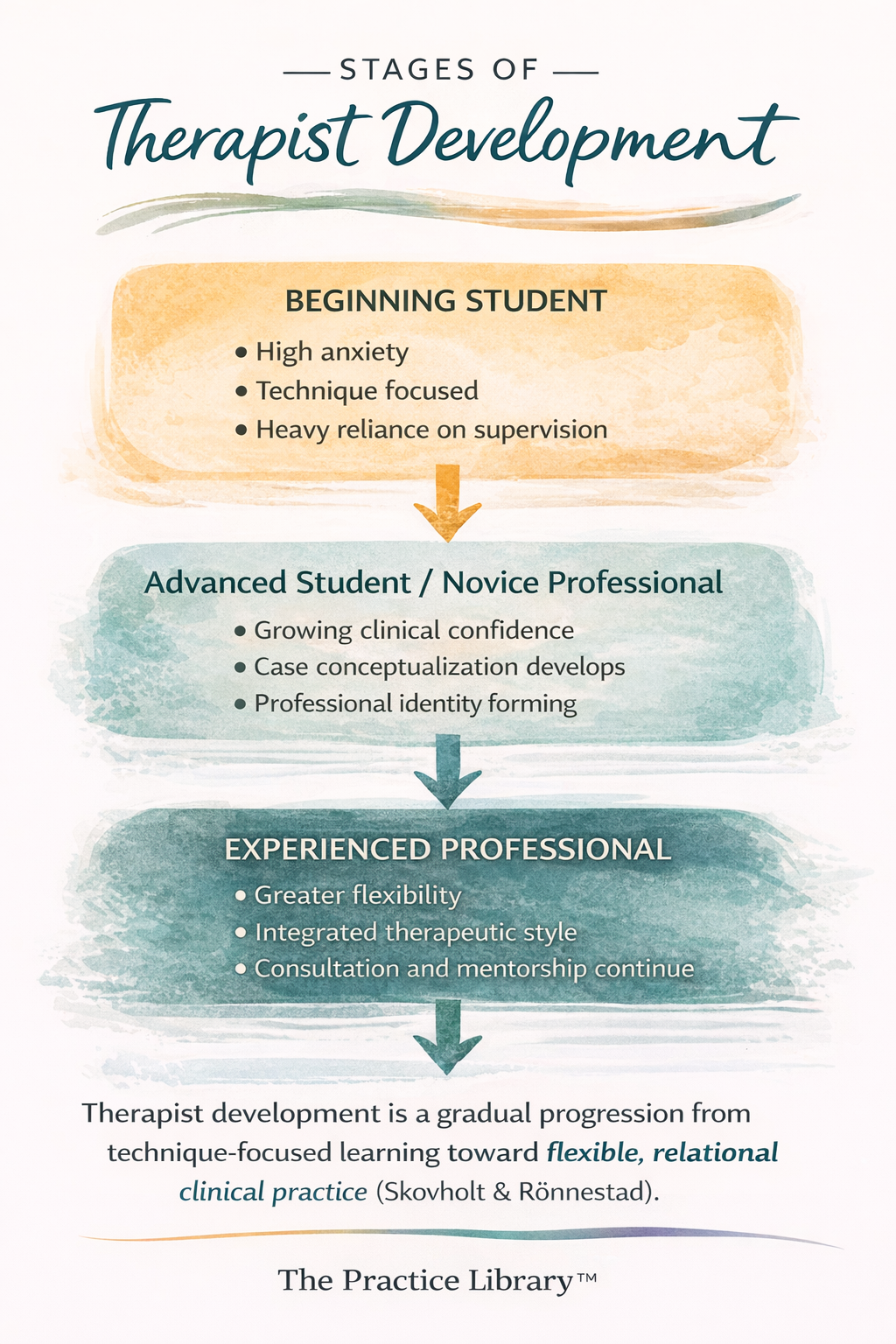
Therapist development is a structured progression—not a personal failure when it feels difficult.
Burnout in the early years is often misunderstood as a failure of resilience. More accurately, it reflects predictable developmental stages.
Stage 1: Anxiety and Technique Reliance
Clinicians lean heavily on models, scripts, and interventions. There is a strong desire to “do it right.”
Stage 2: Searching for Certainty
There is an increased need for clarity, structure, and validation. Ambiguity feels threatening.
Stage 3: Identity Confusion
Clinicians begin to question:
What kind of therapist am I?
What actually works?
Where do I fit?
Stage 4: Integration Begins
Clinical thinking deepens. Flexibility increases. The clinician starts to trust their judgment.
Burnout often emerges when clinicians are expected to perform at Stage 4 while still developing in earlier stages.
Why Burnout Happens (It’s Not Just About Self-Care)
Burnout is frequently framed as an issue of self-care. This framing is incomplete—and, at times, misleading.
In the first five years of practice, burnout is not simply about individual coping capacity. It is the predictable result of developmental demands colliding with system expectations.
We also have to name the workforce reality:
A commonly cited estimate suggests that up to 50–60% of clinicians do not make it from associate status to full licensure (figures vary by discipline and region, but the trend is consistent).
This represents a significant loss of trained clinicians during the exact phase intended for professional development.
This is not a personal failure rate. It is a system retention problem.
“Burnout is not a failure of resilience—it is a failure of alignment.”
The Core Drivers of Early Career Burnout
Burnout in early clinicians is often driven by overlapping and compounding pressures:
1. Developmental Mismatch
Clinicians are expected to function with autonomy and confidence before those capacities are fully developed
Early-stage clinicians are evaluated as if they are later-stage practitioners
2. Inadequate or Misaligned Supervision
Supervision may be overly rigid, compliance-focused, or inconsistent
Limited attention to clinical thinking, identity development, and emotional processing
Mismatch between supervisor development and clinician needs
3. Productivity and Billing Pressures
Expectations tied to billable hours rather than clinical readiness
Limited control over caseload acuity and volume
Pressure to maintain throughput in systems that prioritize access over sustainability
4. Documentation Burden Without Training
High expectations for medical necessity, defensibility, and compliance
Minimal structured training in how to think and write clinically
Documentation becomes a source of anxiety rather than a tool for clinical clarity
5. Emotional Labor Without Containment
Exposure to trauma, crisis, and complex presentations early in practice
Limited structures for processing countertransference and emotional impact
High empathy demands without parallel support systems
The Compounding Risk Profile of the Field
When these factors converge, clinicians are not just at risk for burnout—they are at risk for:
Chronic stress and emotional exhaustion
Imposter syndrome that does not resolve with experience
Ethical distress when unable to provide the level of care they believe is needed
Early exit from the profession despite significant investment in training
This creates a paradox:
We invest heavily in training clinicians, then place them in conditions that make retention difficult.
The System-Level Reality
When clinicians are expected to carry high levels of responsibility without corresponding support, burnout becomes likely—not exceptional.
If more than half of clinicians struggle to reach full licensure, the question is no longer:
“Why are clinicians burning out?”
It becomes:
“What are we asking of clinicians during this phase—and what are we failing to provide?”
Answering that question is essential if we want to retain a sustainable, ethical, and effective behavioral health workforce.
Burnout in clinicians is often less about individual resilience and more about isolation, system pressure, and lack of structured support—patterns explored further in my writing on imposter syndrome, burnout, and workforce sustainability.
The Hidden Financial and Structural Pressures
There is also a financial and structural reality that is often minimized in conversations about the field—and yet, it is central to understanding early career burnout.
After graduate school, clinicians enter a period where they are simultaneously expected to grow, perform, and invest:
Paying for supervision (in many cases)
Earning lower wages as associates
Working toward additional credentials or certifications
At the same time, advanced training in specialized modalities often requires:
Significant financial investment
Time away from clinical work
Ongoing consultation or certification fees
This creates a system where access to advanced clinical identity is shaped not only by interest or aptitude—but by financial capacity, time, and access to opportunity.
The Reality of “Earning Your Place” in the Field
There is an unspoken narrative within the profession that early clinicians must “pay their dues” or “serve their time.”
While there is value in developmental progression, this framing can shift into something more concerning when:
Early career clinicians are underpaid relative to the demands placed on them
Supervision becomes a financial burden rather than a protected developmental space
Training pathways feel inaccessible without significant personal investment
At its worst, this can begin to feel less like professional development—and more like a system that extracts labor and financial resources from those at the earliest stages of their careers.
The Role of Credentialing Bodies—and the Gaps That Remain
Professional organizations such as NASW, ACA, NBCC, and AAMFT play an important role in creating cohesion, ethical standards, and identity within the field.
These structures matter. They provide:
Ethical frameworks
Professional accountability
Shared language across disciplines
And yet, even with these efforts, there are still gaps in how the field supports clinicians during the associate phase.
Standardization does not always translate into accessible, equitable, and developmentally appropriate pathways.
Equity and Access in Professional Development
For clinicians from marginalized communities—including BIPOC and LGBTQIA+ clinicians, and those with lived experience—these barriers can be even more pronounced.
Financial strain, limited access to mentorship, and systemic inequities can impact:
Ability to pursue advanced certifications
Access to high-quality supervision
Opportunities for specialization and leadership
This means that who advances in the field is not solely based on skill or clinical insight—but is also shaped by structural access and resources.
When Development Becomes Transactional
At its best, the associate period should be a time of:
Mentorship
Skill-building
Reflection
Professional identity formation
A period held with a sense of reverence for the responsibility of bringing up a new clinician.
“When growth becomes transactional, sustainability becomes optional”
But when financial pressures, productivity demands, and fragmented training systems dominate, this phase can become:
Transactional
Extractive
Misaligned with its intended purpose
The result is not just burnout—it is a distortion of what early professional development is meant to be.
And ultimately, it contributes to inequity in who is able to remain, grow, and specialize within the field.
These pressures are not separate from workforce sustainability—they are central to it, particularly in how clinicians are supported, compensated, and retained over time.
Gatekeeping, Identity, and Professional Tension
Within the field, there can also be subtle (and sometimes overt) forms of gatekeeping—and early career clinicians are often the ones who feel it most acutely.
Across supervision conversations, professional groups, and online communities where clinicians seek support in what is often a siloed and isolating field, similar themes emerge:
Uncertainty about what is “allowed” versus what is “owned” by a modality
Fear of being criticized for using interventions outside of formal certification
Confusion about how to ethically integrate creativity, relational work, and evidence-based practice
Clinicians may encounter tensions such as:
Criticism for using creative or expressive interventions without formal specialty credentials
Rigid interpretations of modality ownership
Hierarchies based on certification status
Examples frequently shared include:
Concerns from art therapists when art is used without formal art therapy credentials
Pushback from music therapists regarding the use of music in sessions
Tension around play-based approaches in school or clinical settings
Policing of language around modalities (e.g., whether one can “say” they are using a specific approach)
The Impact on Developing Clinicians
For early clinicians—already navigating anxiety, identity formation, and a desire to practice ethically—these dynamics can have a disproportionate impact.
They can lead to:
Increased self-doubt and second-guessing
Over-reliance on rigid techniques rather than clinical judgment
Fear-based decision-making rather than thoughtful integration
Hesitation to explore creativity or relational depth in clinical work
They also intersect with broader structural pressures in ways that intensify imposter syndrome and financial strain:
A growing belief that one is "not qualified enough" without additional certifications
Pressure to pursue costly trainings early in development to feel legitimate
Confusion between ethical scope of practice and credential-based permission
Internalization of the idea that confidence must be earned through external validation rather than supervised experience
This can create a subtle but powerful “pay-to-play” dynamic, where:
Legitimacy feels tied to financial investment in modalities and credentials
Clinicians feel behind if they cannot afford advanced trainings
Professional identity becomes shaped by access to resources rather than developmental readiness
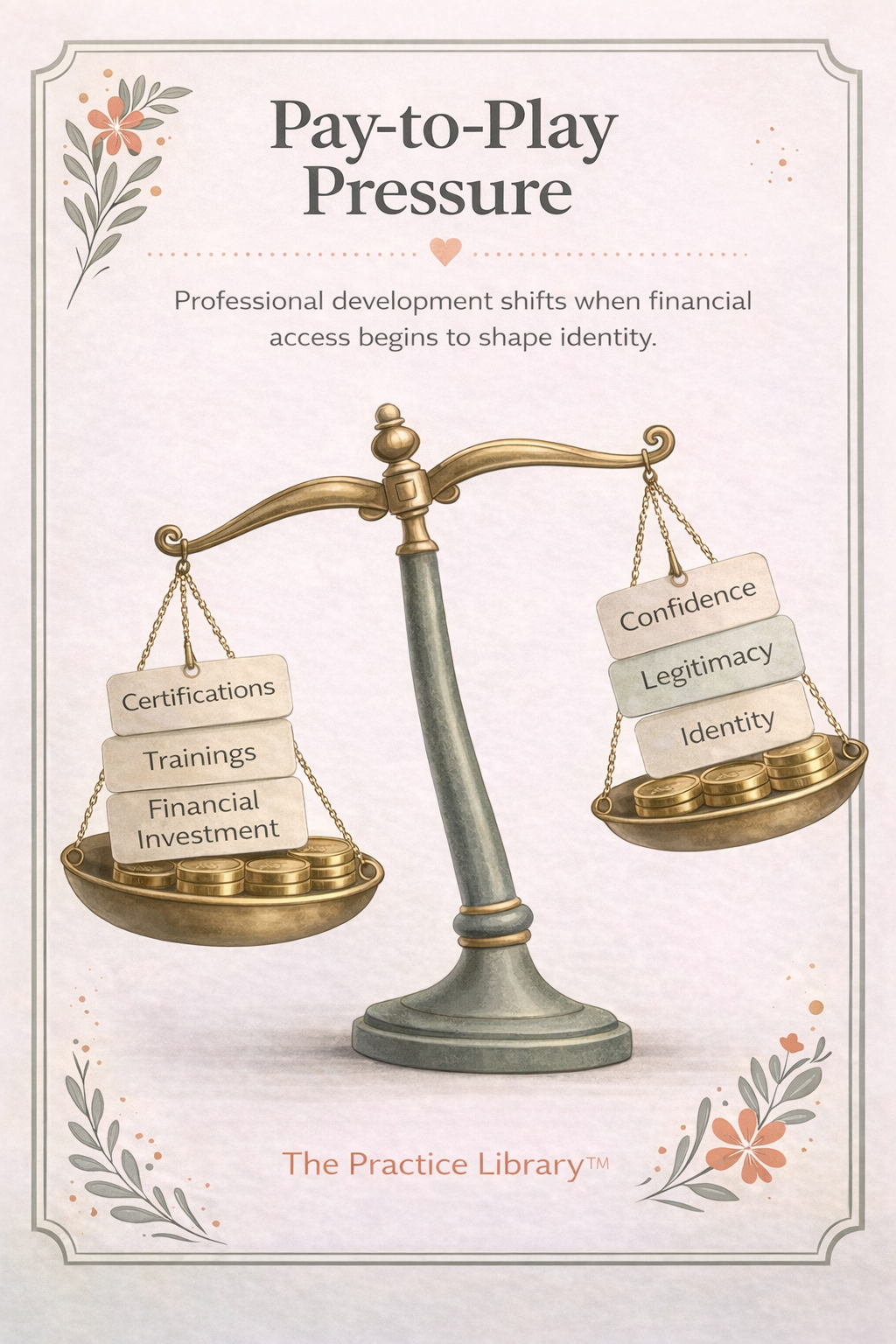
When professional identity becomes tied to financial access, development can shift from growth to comparison.
At the same time, many clinicians are:
Paying for supervision
Working toward licensure requirements
Managing lower associate-level wages
The result is a convergence of financial pressure, identity insecurity, and professional comparison during an already vulnerable stage of development.
“When legitimacy is tied to access, confidence becomes conditional.”
In a field that requires flexibility, attunement, and responsiveness, this kind of pressure can narrow clinical thinking and inadvertently slow development.
Specialization vs. Ownership
It is important to be clear: specialization and advanced training matter.
They deepen skill, protect client care, and ensure ethical use of complex interventions.
At the same time, there is a meaningful distinction between:
Respecting specialized training, and
Restricting foundational therapeutic tools as if they are exclusively owned
Many core elements of therapy—such as creativity, relationship-building, emotional expression, and symbolic work—are not owned by any single modality.
When these are treated as proprietary, it can create unnecessary division within the field.
When Legitimacy Becomes Transactional
For some clinicians, these experiences reinforce a deeper message:
That legitimacy must be purchased, credentialed, or externally validated—rather than developed through ethical, reflective, and supervised practice.
This can intersect with the financial and structural pressures already present in early career development, further intensifying:
Financial strain
Professional insecurity
Barriers to identity formation
A Field-Level Reflection
These patterns are not simply interpersonal—they reflect broader questions within the profession:
How do we balance specialization with accessibility?
How do we maintain standards without creating unnecessary barriers?
How do we support innovation and integration while honoring training and expertise?
For developing clinicians, navigating these tensions without clear guidance can contribute to both burnout and confusion about their role in the field.
For the profession, it raises an important consideration:
Are we creating pathways that support growth—or reinforcing structures that make clinicians feel like they must constantly prove their legitimacy?
Addressing this tension is part of building a more sustainable, collaborative, and developmentally attuned clinical workforce.
What Actually Supports Sustainability
If burnout is not simply an individual issue, then sustainability requires more than individual solutions.
What actually supports clinicians in the first five years includes:
High-Quality Supervision
Supervision that supports clinical thinking, not just case review.
Documentation Competence
Understanding how to document clearly, ethically, and in alignment with medical necessity reduces cognitive load and anxiety.
Realistic Caseload Development
Gradual exposure to complexity, rather than immediate overload.
Peer Consultation and Community
Reducing isolation and increasing shared learning.
Systems Awareness
Understanding how healthcare systems, reimbursement, and policy shape clinical work.
A Necessary Reframe
Burnout in the first five years is not simply a failure of the individual clinician.
It is often a signal:
That development is being rushed
That systems are outpacing support
That expectations are misaligned with reality
If we want to retain clinicians, we have to shift how we understand this phase.
Not as a proving ground—but as a developmental period that requires structure, investment, and care.
Bringing It All Together
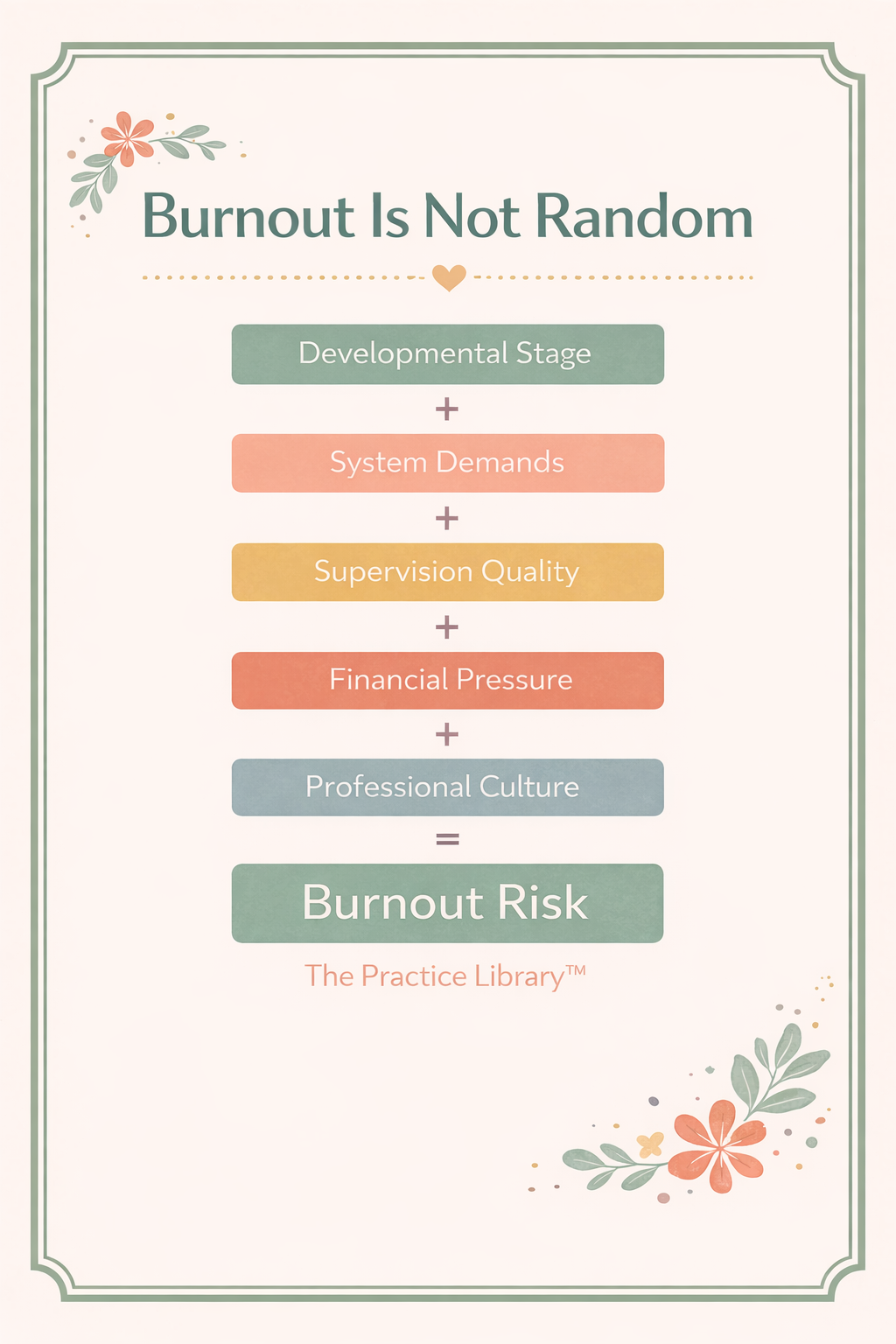
Burnout is not random—it emerges when multiple systems place demand on a clinician without aligned support.
When we step back, a clearer picture emerges.
Early career burnout is not caused by a single factor—it is the result of multiple systems interacting at once:
Clinicians developing through predictable stages of professional identity formation
Expectations to perform within complex clinical and documentation systems
Variable access to high-quality, developmentally aligned supervision
Significant financial and structural pressures during the associate phase
Professional cultures that can unintentionally reinforce gatekeeping and pay-to-play dynamics
When these systems are aligned, clinicians are supported in becoming thoughtful, skilled, and sustainable practitioners.
When they are misaligned, clinicians are asked to carry more than their developmental stage can reasonably hold.
Burnout, in this context, is not random.
It is the predictable outcome of a system that asks for advanced clinical performance without consistently providing the developmental, relational, and structural support required to sustain it.
If we want to meaningfully address workforce attrition, we must shift from asking clinicians to adapt to these conditions—
and instead begin redesigning the conditions themselves.
Nonlinear Development and Transitions
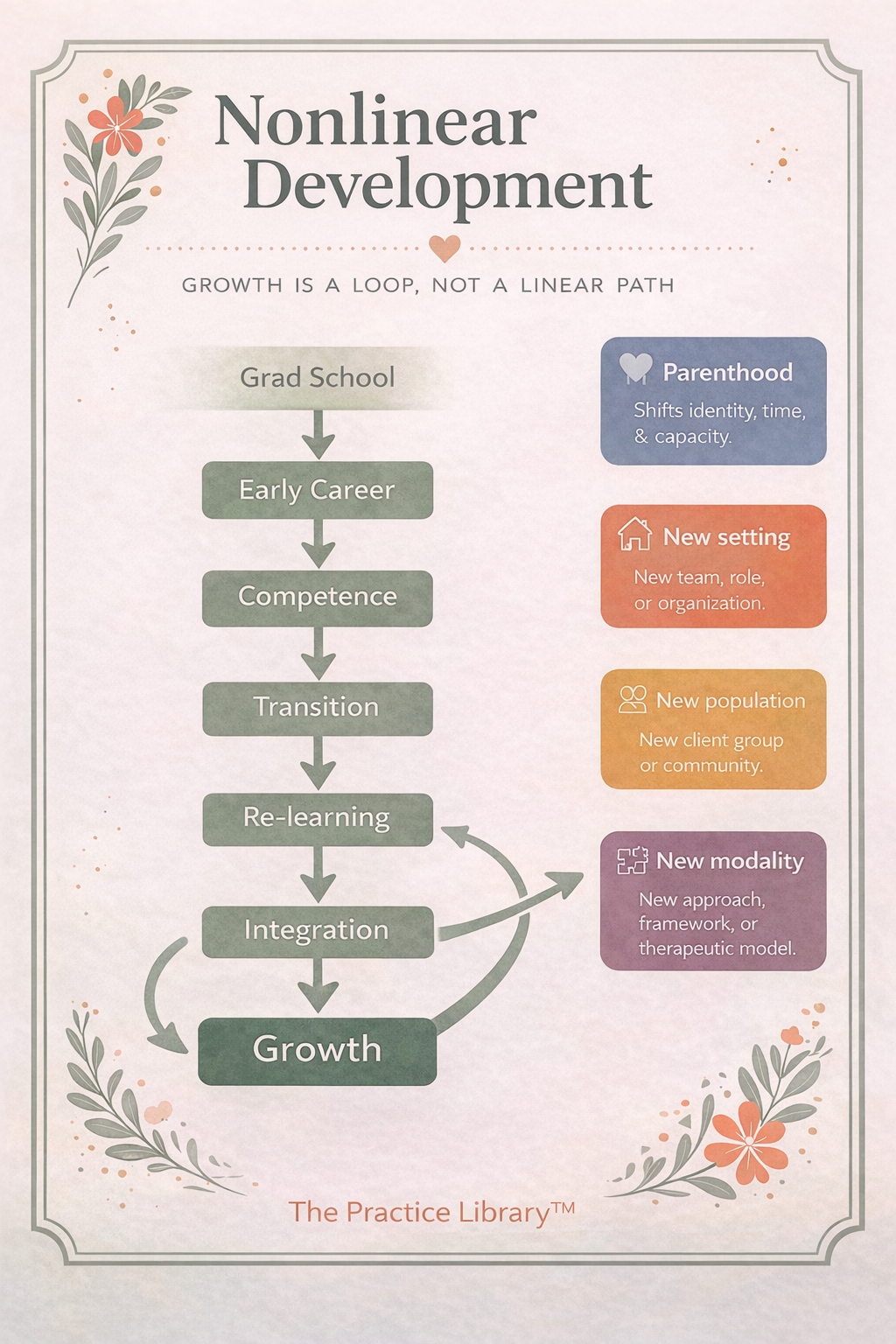
Clinical development is not linear—transitions reintroduce learning curves across a career.
The first five years are often described as a linear progression—but in practice, clinician development is rarely linear.
Life events and professional shifts—such as becoming a parent, changing service settings, or moving between populations (community mental health, crisis, forensics, medical, schools, private practice; adults to older adults; birth-to-five to adolescents)—reintroduce learning curves that can echo earlier developmental stages.
Clinicians may find themselves:
Rebuilding confidence in a new context
Adapting clinical thinking to different systems and documentation expectations
Renegotiating identity as their roles and responsibilities evolve
These transitions do not reset development to zero, but they do require new integration. The timeline to feel grounded may be shorter than the initial years—but the need for support, mentorship, and space to learn remains real. These transitions mirror the same developmental processes seen in early career clinicians, reinforcing that support and structured reflection remain essential across the lifespan of a clinician’s career.
“The first five years don’t always happen in the first five years.”
This has implications for how we think about burnout and support:
Development is ongoing and context-dependent, not confined to a fixed window
Transitions are predictable stress points, not personal setbacks
Support structures should follow the clinician, not end once hours are completed
There is also a professional responsibility embedded here.
In a field where the work itself is already demanding, clinicians rely on one another to create environments that are:
Collaborative rather than competitive
Mentoring rather than gatekeeping
Expansive rather than isolating
If we recognize that development continues across settings, roles, and life stages, then supporting one another is not optional—it is essential to sustaining the field itself.
Final Thought
We ask a great deal of clinicians before they are fully formed in their professional identity.
If we continue to treat burnout as an individual weakness, we will continue to lose clinicians.
If we begin to understand it as a predictable outcome of developmental and systemic pressure, we have an opportunity to build something different.
The work is already hard. Supporting one another in doing it should not be.
“If we want to sustain clinicians, we have to build systems that develop them—not just demand from them.”
References & Further Reading
This article reflects both published research and clinical experience within behavioral health systems. The following sources provide additional context on clinician development, supervision, burnout, and workforce sustainability.
Morse, G., Salyers, M. P., Rollins, A. L., Monroe-DeVita, M., & Pfahler, C. (2012). Burnout in mental health services: A review of the problem and its remediation. Administration and Policy in Mental Health and Mental Health Services Research, 39(5), 341–352.
Rupert, P. A., & Morgan, D. J. (2005). Work setting and burnout among professional psychologists. Professional Psychology: Research and Practice, 36(5), 544–550.
Health Resources and Services Administration (HRSA). (2023). Behavioral Health Workforce Projections.
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM Supervision: An Integrative Developmental Model for Supervising Counselors and Therapists.
Bernard, J. M., & Goodyear, R. K. (2018). Fundamentals of Clinical Supervision.
Figley, C. R. (1995). Compassion Fatigue: Coping with Secondary Traumatic Stress Disorder in Those Who Treat the Traumatized.
Newell, J. M., & MacNeil, G. A. (2010). Professional burnout, vicarious trauma, secondary traumatic stress, and compassion fatigue.
Gibson, D. M., Dollarhide, C. T., & Moss, J. M. (2010). Professional identity development: A grounded theory of transformational tasks of new counselors.
National Association of Social Workers (NASW). (2021). Code of Ethics.
SAMHSA. (2022–2024). Behavioral Health Workforce Reports.
American Psychological Association (APA). (2023). Stress in America Survey.
Related Articles from The Practice Library™
SB Webb Counseling & Consulting PLLC | The Practice Library™
Clinical supervision and consultation with integrity, structure, and relational mentorship.
sbwebbcounselingconsulting.org
If you are a clinician navigating these early or transitional stages of practice and are seeking structured, reflective supervision or consultation, you can learn more about working with me here.
Stay Connected
I share articles, clinical reflections, and supervision resources periodically through The Practice Library.
If you’d like to stay connected, you’re welcome to follow along or join for updates.