

The Supervision Ecosystem: Why Therapists Develop Through Community, Not Supervision Alone
Part of The Practice Library™ series on clinical supervision, therapist development, and behavioral health systems.
SB Webb Counseling & Consulting PLLC | The Practice Library™
sbwebbcounselingconsulting.org
In conversations about therapist development, clinical supervision is often treated as the primary mechanism through which clinicians learn the work.
This framing is not inaccurate.
Clinical supervision is one of the primary professional structures through which therapists develop clinical judgment, ethical decision-making, and a stable professional identity over time.
It is where many clinicians begin integrating theory, documentation, ethics, and real-world complexity into a functional professional practice.
But it is incomplete.
Because therapists do not develop through supervision alone.
They develop within a broader network of professional relationships, structures, and experiences that shape how they think clinically, practice ethically, and sustain themselves over time.
“Therapists do not develop through supervision alone. They develop through the systems that support how they think, reflect, and practice over time.”
If we return to the question raised in the previous article - how therapists actually learn the work - we are led to a more expansive understanding:
Clinical development does not occur within a single relationship.
It occurs within what can be understood as a supervision ecosystem.
Defining the Supervision Ecosystem
The supervision ecosystem refers to the interconnected network of professional supports that contribute to therapist development over time.
While supervision literature has long recognized the administrative, educational, and supportive functions of supervision, these models primarily focus on what occurs within the supervisory relationship itself.
The Supervision Ecosystem Model, developed by Shannon Webb, LICSW, founder of SB Webb Counseling & Consulting and creator of The Practice Library™, extends this perspective by accounting for the broader network of relationships and systems through which clinicians develop in real-world practice.
While supervision remains central, it functions alongside other forms of support that help clinicians build competence, flexibility, and professional identity.
This network typically includes:
clinical supervision
peer consultation
mentorship
documentation and clinical thinking systems
organizational and systems support
Each of these elements serves a distinct function.
Together, they create the conditions under which clinicians develop competence, confidence, consistency, and professional identity.
“Supervision is essential, but it is not the system. It is one part of a larger structure that supports clinical development.”
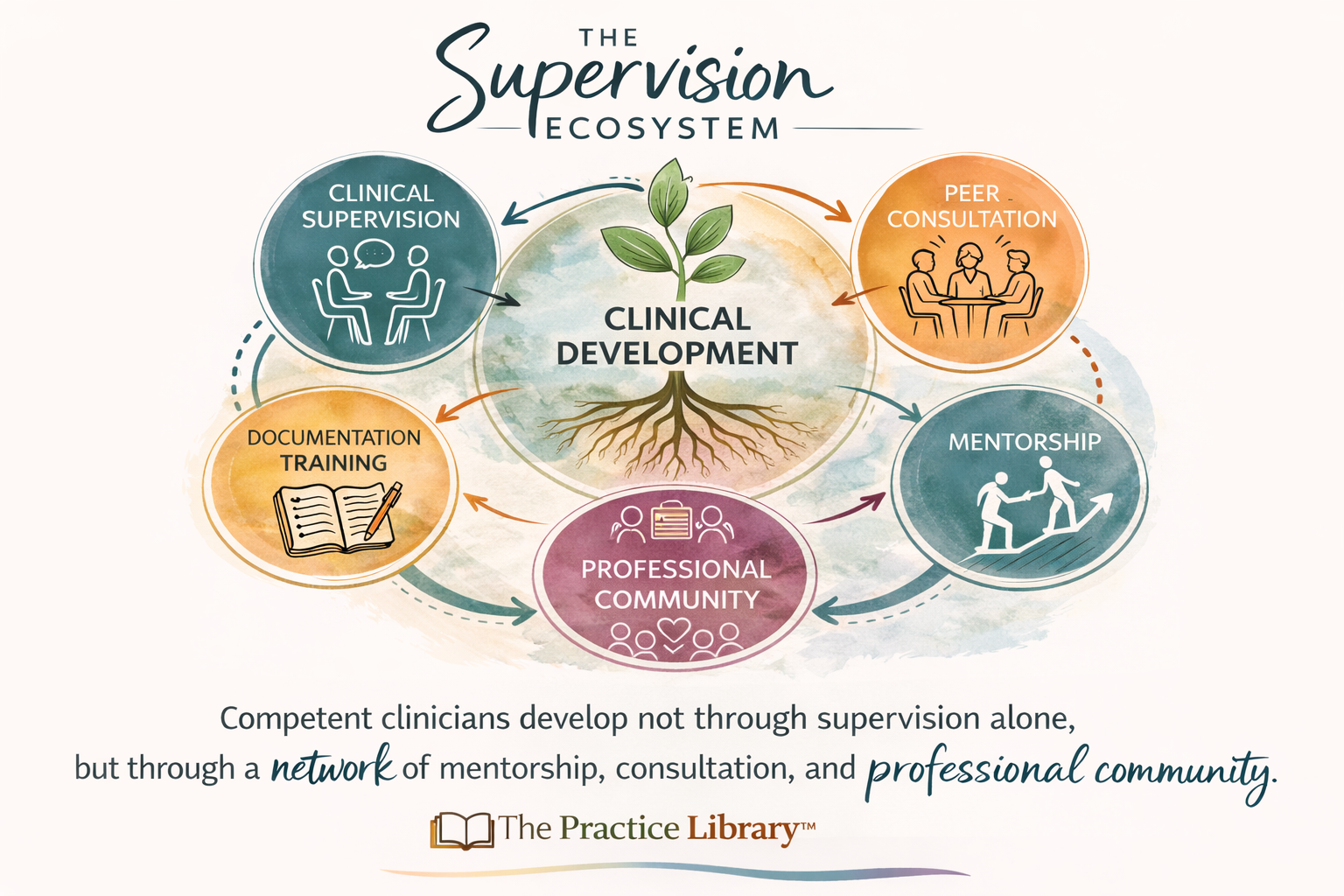
The Supervision Ecosystem Model
As developed by Shannon Webb, LICSW, clinicians develop through interconnected systems of support, not supervision alone.
The Practice Library™ | Shannon Webb, LICSW | SB Webb Counseling & Consulting
While supervision remains a central component, it is only one part of a larger developmental system.
Understanding this distinction is critical.
Because when we expect supervision alone to carry the full weight of clinician development, we place unrealistic demands on both supervisors and supervisees — and we risk overlooking the broader structures that shape clinical practice.
We also risk confusing the limits of a system with the limits of a clinician.
“When we over-rely on supervision, we often overlook the systems that shape clinical practice.”
The Core Components of the Ecosystem
Clinical Supervision: Structure and Accountability
Clinical supervision provides the formal structure through which clinicians receive guidance, feedback, and evaluation.
It is one of the primary environments in which therapists begin integrating theory, documentation, ethical standards, and real-world clinical complexity into a functional professional practice.
It is where therapists learn to:
connect assessment to diagnosis
develop and refine treatment plans
strengthen documentation
navigate ethical decision-making
reflect on clinical interactions
tolerate uncertainty in complex cases
Supervision also serves an essential gatekeeping function, ensuring that clinical work meets professional and ethical standards (Bernard & Goodyear, 2019).
However, supervision is inherently constrained by its role.
It is both supportive and evaluative.
It is time-limited.
And it must balance multiple competing functions within a single relationship.
These conditions shape how supervision operates in practice.
Supervisors must attend simultaneously to clinical development, risk management, documentation quality, ethical oversight, and organizational expectations—often within a limited amount of time.
For that reason, even excellent supervision cannot be expected to meet every developmental need a clinician brings to the work.
“Supervision provides structure, but it cannot carry the full weight of development”
Peer Consultation: Collaborative Clinical Thinking
While supervision includes evaluation, peer consultation offers something different.
It provides a non-evaluative space where clinicians can:
explore uncertainty
test clinical hypotheses
compare conceptualizations
process difficult cases
normalize the ambiguity and complexity of clinical work
Research and supervision literature consistently emphasize the importance of collegial dialogue in developing clinical reasoning and reducing professional isolation (Hill & Knox, 2013).
Peer consultation allows clinicians to think out loud in ways that are not always possible within evaluative supervisory relationships.
In these spaces, clinicians are often able to examine their assumptions more openly, consider alternative perspectives, and engage more fully in the process of clinical reasoning.
It is often where clinical thinking becomes more flexible, creative, and integrative.
“Clinical thinking develops in dialogue not in isolation.”
Over time, this process helps clinicians move away from searching for a single “correct” intervention and toward a more nuanced understanding of client experience.
It can also be where clinicians begin to recognize that there is rarely a single correct way to understand a case.
Mentorship: Professional Identity Development
Mentorship extends beyond case discussion.
It supports the development of professional identity, long-term career direction, and the integration of personal values with professional role.
Developmental models of therapist growth highlight that clinicians evolve not only in skill, but in how they understand themselves in the role of therapist (Skovholt & Rønnestad, 2013).
Mentorship helps clinicians navigate questions such as:
What kind of clinician am I becoming?
How do I sustain myself in this work over time?
How do I align my values with my practice?
Documentation and Clinical Thinking Systems
One of the most overlooked components of therapist development is how clinicians organize their thinking.
As explored in previous Practice Library articles, documentation is not simply administrative work.
“Documentation is not separate from clinical work, it is the written expression of how clinicians think.”
Systems that support strong documentation - including training, feedback, and structured frameworks - help clinicians:
Without these systems, clinicians may struggle to translate their clinical intuition into defensible, coherent documentation.
In practice, this often means clinicians know more than they can clearly articulate in the record. Over time, that gap can affect confidence, continuity of care, audit readiness, and the ability to communicate clinical reasoning across settings.
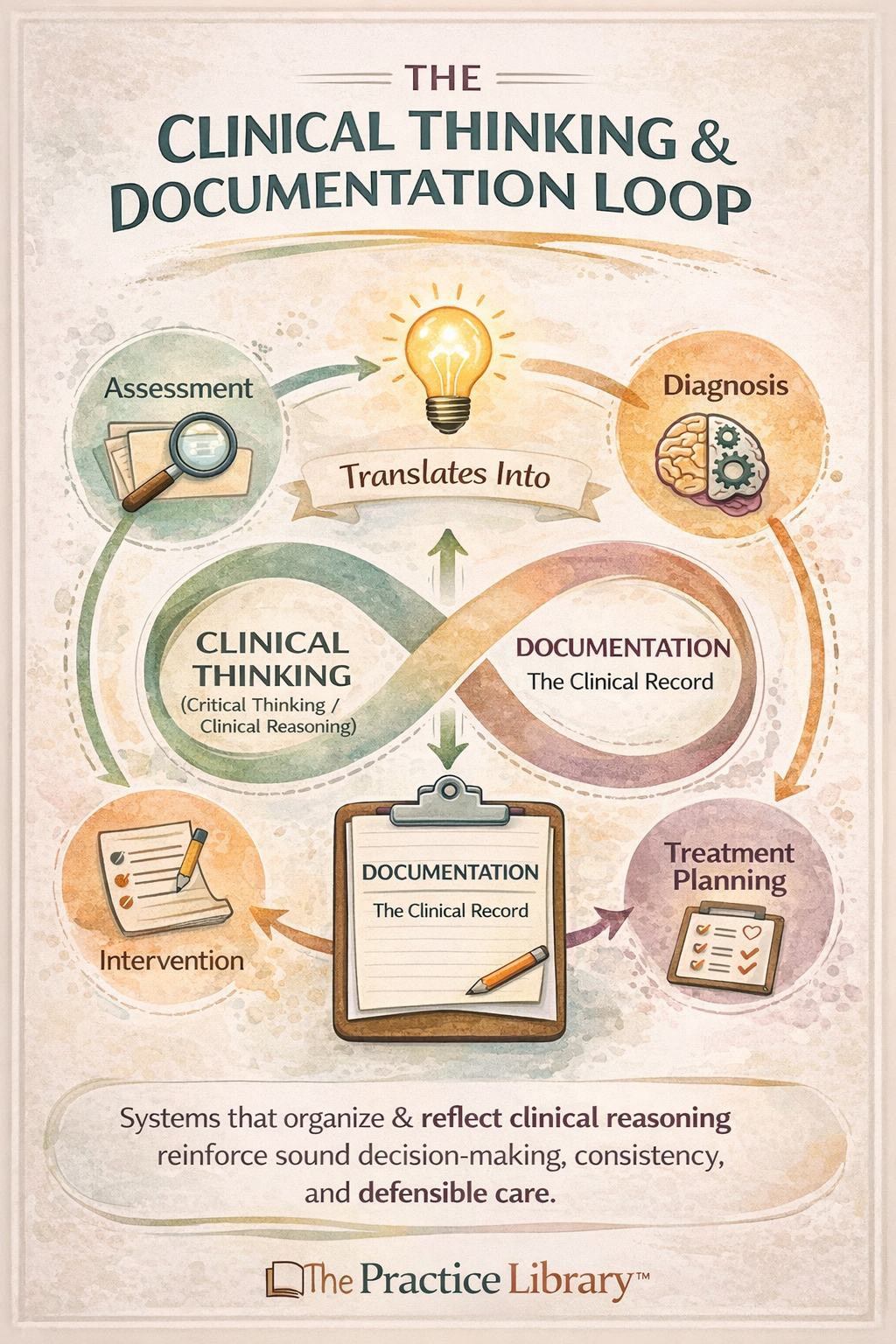
The Clinical Thinking & Documentation Loop
Documentation is the written expression of clinical reasoning, shaping and strengthening clinical thinking over time.
The Practice Library™ | Shannon Webb, LICSW | SB Webb Counseling & Consulting
Documentation, in this sense, functions both as a developmental tool and as visible evidence of clinical competence.
Clinical competence is not only developed - it is supported by the systems in which clinicians practice.
“Clinical thinking is strengthened when it is made visible, structured, and revisited over time.”
Organizations and Systems: The Environment That Shapes Practice
Clinicians do not practice in a vacuum.
“Clinician performance is not only an individual outcome, it is shaped by the systems in which clinicians practice.”
Organizational structures — including productivity expectations, caseload size, access to consultation, and workplace culture — significantly influence how therapists develop.
Environments that:
limit access to consultation
prioritize productivity over reflection
minimize supervision time
fail to support documentation development
can constrain development, even when individual supervisors are highly skilled.
Conversely, environments that support collaboration, reflection, and ongoing learning create conditions where clinicians are more likely to grow and remain in the field.
This is part of what it means to treat workforce development as a systems responsibility rather than an individual burden.
What Happens When the Ecosystem Is Incomplete
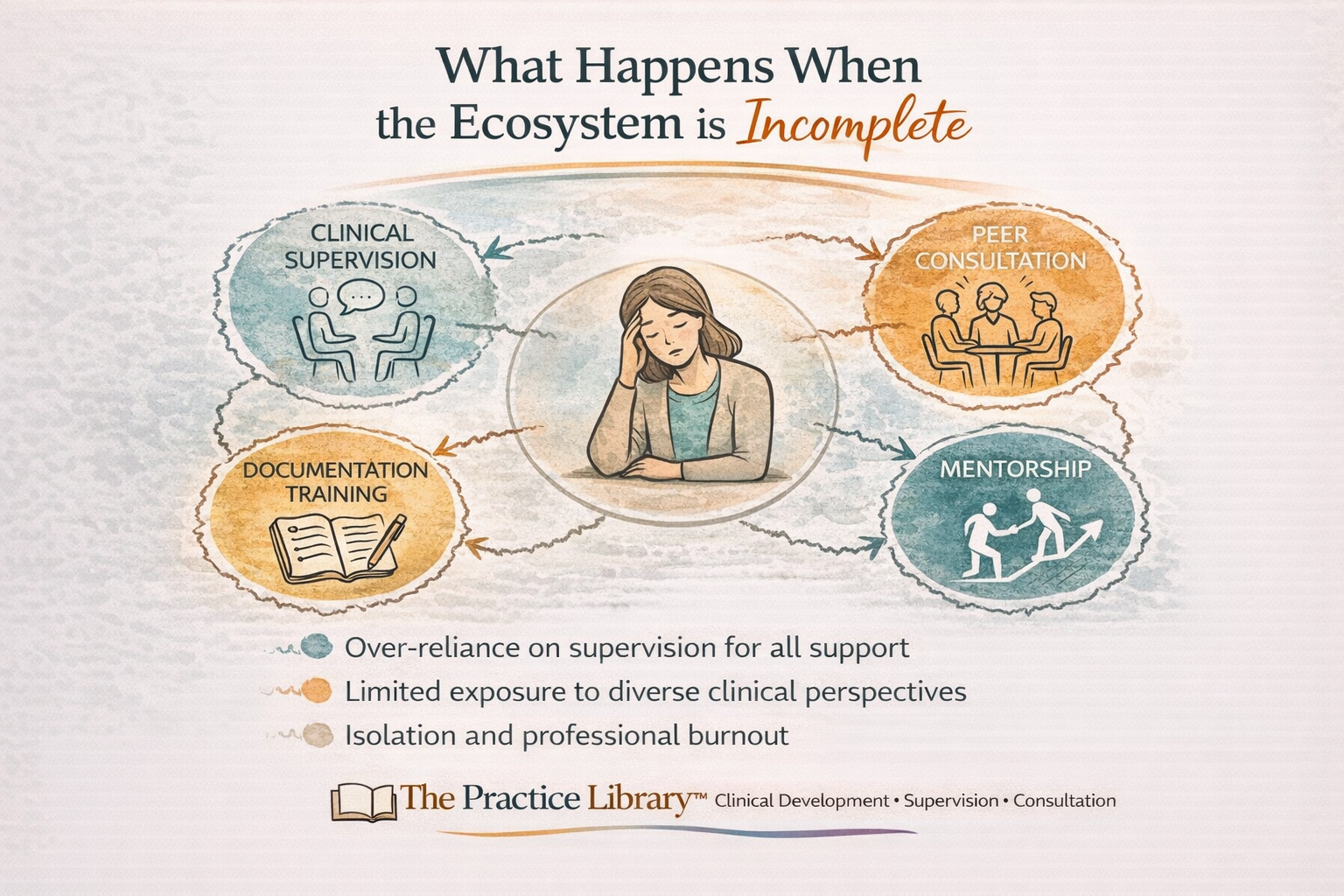
When the Supervision Ecosystem Is Incomplete
Clinicians may experience isolation, burnout, and stalled development when key supports are missing from their professional environment.
The Practice Library™ | Shannon Webb, LICSW | SB Webb Counseling & Consulting
“When support structures are missing, clinicians often struggle, not because they are unskilled, but because they are under-supported.”
When key elements of the supervision ecosystem are missing, clinicians often experience predictable challenges:
over-reliance on supervision for all forms of support
limited exposure to diverse clinical perspectives
difficulty developing independent clinical judgment
professional isolation
increased risk of burnout
self-doubt that is reinforced by structural rather than clinical gaps
Early-career clinicians, in particular, may struggle when supervision is expected to function as:
instructor
mentor
colleague
source of professional containment
system navigator
No single relationship can sustainably hold all of these roles.
Why Supervision Alone Is Not Enough
Clinical supervision is essential.
But it is not designed to meet every developmental need.
Supervisors operate within defined roles that include:
evaluation
ethical oversight
organizational accountability
These responsibilities shape the supervisory relationship in important ways.
For example:
supervisees may hesitate to disclose uncertainty due to evaluation concerns
time constraints limit the depth of clinical exploration
supervision must balance multiple priorities within each session
Because of these constraints, supervision is both supportive and evaluative, structured and limited.
It is designed to guide clinical work, ensure ethical practice, and support development within a defined scope.
Supervision can support clinical thinking.
But it cannot fully replace the functions of peer dialogue, mentorship, or broader professional community.
It cannot be the only place where clinicians process complexity, test ideas, and develop professional identity over time.
Recognizing this limitation is not a critique of supervision.
It is a recognition of its scope.
“Supervision is essential, but it is not meant to stand alone.”
And, importantly, a recognition that effective supervision depends on the presence of a broader ecosystem of support.
Reframing Responsibility: From Supervision to Systems
When clinicians struggle, the response is often to ask:
“Is supervision adequate?”
A more useful question may be:
“What does the clinician’s supervision ecosystem look like?”
This shift matters.
“The question is not whether supervision is enough. The question is what system surrounds it.”
Because it moves the focus from evaluating a single relationship to examining the broader system of support surrounding the clinician.
It reframes development as a shared responsibility across:
supervisors
organizations
professional communities
clinicians themselves
Rather than placing the burden of growth on supervision alone, this perspective recognizes that clinical development is shaped by multiple, interacting structures.
It also highlights the need to intentionally build environments that support development beyond formal supervision.
That may include:
consultation networks that allow for collaborative clinical thinking
documentation training that strengthens clinical reasoning and clarity
reflective team cultures that support ongoing dialogue and learning
mentorship relationships that guide long-term professional development
access to practice support beyond individual supervision hours
When these structures are present, clinicians are more likely to develop with confidence, flexibility, and consistency.
When they are absent, supervision is often asked to carry more than it was designed to hold.
Reframing responsibility in this way is not about reducing the importance of supervision.
It is about recognizing that supervision functions most effectively when it is part of a broader, well-supported system of care.
Practical Implications
-
Organizations play a critical role in shaping the conditions under which clinicians develop. Clinical competence is not only an individual achievement - it is influenced by the structures, expectations, and supports embedded within the system of care.
This may include:
Creating structures for peer consultation and case discussion
Establishing regular opportunities for clinicians to engage in collaborative clinical thinking, share perspectives, and reduce isolation through team-based or interdisciplinary consultation.Protecting time for supervision and clinical reflection
Ensuring that supervision is not consistently deprioritized in response to productivity demands, and that clinicians have dedicated space to reflect on clinical work, decision-making, and ethical considerations.Recognizing documentation as a clinical skill, not just a compliance task
Supporting a culture in which documentation is understood as the written expression of clinical reasoning, rather than solely an administrative requirement.Supporting access to training that strengthens diagnostic reasoning and documentation quality
Providing ongoing learning opportunities that help clinicians connect assessment, diagnosis, treatment planning, and intervention into a coherent clinical framework.Aligning productivity expectations with ethical clinical practice
Evaluating whether caseloads, scheduling expectations, and documentation requirements allow clinicians sufficient time to think, reflect, and provide quality care.Expanding access to supervision, consultation, and mentorship structures
Recognizing that supervision alone is not sufficient, and investing in broader systems of support that contribute to clinician development and retention.
Organizations do not just employ clinicians.
They shape the environments in which clinical thinking develops - or is constrained.
-
Supervisors play a central role in clinician development, but that role exists within a broader ecosystem of support. Effective supervision includes not only guiding clinical work, but also helping clinicians understand how to build sustainable professional structures beyond supervision itself.
This may include:
Encouraging supervisees to seek additional consultation
Supporting clinicians in building relationships outside of supervision, including peer consultation groups and mentorship connections that broaden perspective and reduce over-reliance on a single supervisory relationship.Supporting development beyond immediate case management
Moving beyond session-by-session review to focus on clinical reasoning, case conceptualization, documentation quality, and the development of independent clinical judgment over time.Recognizing the limits of the supervisory role
Acknowledging that supervision cannot function as the sole source of clinical, emotional, and professional support, and helping clinicians identify additional resources when needed.Helping clinicians distinguish between clinical uncertainty and structural under-support
Assisting supervisees in understanding when challenges are part of normal clinical development versus when they are related to gaps in supervision, consultation, workload, or organizational conditions.Modeling clinical thinking and reflective practice
Making your own clinical reasoning visible, demonstrating how experienced clinicians approach complexity, ambiguity, and ethical decision-making.Supporting the development of documentation as a clinical skill
Helping clinicians connect their clinical thinking to their documentation, reinforcing that the clinical record reflects reasoning, not just compliance.
Supervision is not only about guiding clinical work in the moment.
It is about helping clinicians develop the capacity to think, reflect, and practice independently within a broader professional ecosystem.
-
Clinical development is an active, ongoing process that extends beyond formal supervision. Clinicians play an important role in shaping the professional environments and support systems that sustain their growth over time.
This may include:
Building networks of consultation and mentorship
Developing relationships with colleagues and experienced clinicians who can provide perspective, challenge clinical thinking, and support ongoing development.Seeking diverse perspectives
Engaging with clinicians from different disciplines, theoretical orientations, and practice settings to broaden case conceptualization and avoid overly narrow approaches to clinical work.Engaging in ongoing professional development
Participating in trainings, consultation groups, and learning opportunities that strengthen clinical reasoning, ethical decision-making, and specialized areas of practice.Treating documentation as part of clinical development, not separate from it
Approaching documentation as a tool for organizing and refining clinical thinking, rather than as an administrative task to complete after the session.Recognizing when additional support is needed
Identifying gaps in supervision, consultation, or mentorship and taking steps to build a more complete support system.
Clinical competence does not develop passively.
It develops through intentional engagement with the structures, relationships, and practices that support clinical thinking over time.
-
Private practitioners often experience a high degree of clinical autonomy, but that autonomy can also come with increased responsibility for creating and maintaining professional support structures.
Unlike agency or group practice settings, private practice does not automatically provide access to supervision, consultation, or collaborative clinical environments. As a result, clinicians must often build their own supervision ecosystem intentionally.
This may include:
Intentionally creating consultation networks
Developing relationships with trusted colleagues for regular case consultation, rather than relying on informal or inconsistent support.Participating in peer consultation groups
Engaging in structured, ongoing consultation spaces that allow for shared clinical thinking, exposure to diverse perspectives, and reduced professional isolation.Seeking mentorship beyond supervision
Identifying experienced clinicians who can support professional identity development, long-term career decisions, and navigation of complex clinical or ethical situations.Investing in documentation and clinical thinking development
Treating documentation as a core clinical skill, and seeking training or consultation that strengthens diagnostic reasoning, case conceptualization, and audit-ready documentation.Avoiding reliance on a single supervisory relationship
Recognizing that no single relationship can meet all professional needs, and intentionally diversifying sources of support across supervision, consultation, mentorship, and community.
In private practice, building a supervision ecosystem is not automatic.
It is a deliberate part of ethical and sustainable clinical practice.
Supervision as Part of a Larger Professional Infrastructure
As discussed in the previous article, supervision is a critical component of the professional infrastructure that sustains ethical clinical practice.
This article extends that idea.
Supervision does not stand alone.
It functions within a broader ecosystem that supports:
clinical reasoning
professional identity
ethical practice
long-term sustainability in the field
When that ecosystem is strong, clinicians are more likely to develop with confidence, flexibility, and resilience.
When it is fragmented, clinicians may struggle - not due to lack of ability, but due to lack of support.
Transforming How We Think About Development
If we want to uplift the profession, we must support the clinicians doing the work.
If we want to defend the workforce, we must recognize that development does not occur in isolation.
And if we want to transform our systems, we must move beyond the idea that supervision alone is sufficient.
“Therapists do not develop through a single relationship. They develop through community.”
Therapists develop through relationships and the communities that support them.
Through conversation.
Through reflection.
Through shared thinking over time.
The supervision ecosystem is not an abstract concept.
It is the system that supports how clinicians learn to think, document, and practice in real-world settings.
And when that system is strong, it does more than support individual clinicians.
It strengthens the integrity, quality, and sustainability of care across the profession.
Therapists do not learn the work in a single room. They develop through connection, reflection, and the systems that support how they think, practice, and grow.
References
Bernard, J. M., & Goodyear, R. K. (2019). Fundamentals of clinical supervision (6th ed.). Pearson.
Hill, C. E., & Knox, S. (2013). Training and supervision in psychotherapy. In M. J. Lambert (Ed.), Bergin and Garfield's handbook of psychotherapy and behavior change (6th ed.). Wiley.
Maslach, C., & Leiter, M. P. (2016). Burnout: A multidimensional perspective. In Stress: Concepts, cognition, emotion, and behavior. Academic Press.
Skovholt, T. M., & Rønnestad, M. H. (2013). The developing practitioner: Growth and stagnation of therapists and counselors. Routledge.
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors and therapists (3rd ed.). Routledge.
SB Webb Counseling & Consulting PLLC | The Practice Library™
Clinical supervision and consultation with integrity, structure, and relational mentorship.
sbwebbcounselingconsulting.org
Interested in strengthening your supervision ecosystem or clinical documentation practices?