

Uplift the Workforce: Why Clinical Supervision Is More Than Oversight
Therapist Development, Clinical Supervision, and the Professional Community That Sustains the Profession
SB Webb Counseling & Consulting PLLC | The Practice Library™
sbwebbcounselingconsulting.org
Social Work Month invites us to reflect on the profession’s theme this year: Uplift. Defend. Transform.
These words carry weight. They remind us that social work has always been about more than individual clinical encounters. It is about strengthening the systems that support both clients and the professionals who serve them.
But if we take this theme seriously, we must also ask a harder question:
How well are we supporting the clinicians entering the profession today?
In previous Practice Library articles - including Who Helps the Helpers?, Who Holds the Helpers?, and Beyond Imposter Syndrome: Supervision, Community, and the Workforce We’re Building- I explored the emotional toll of clinical work and the structural pressures shaping modern behavioral health systems.
This article turns to another critical piece of the conversation: clinical supervision and therapist development.
Clinical supervision is one of the primary professional structures through which therapists develop clinical judgment, ethical decision-making, and a stable professional identity over the course of their careers.
Because if we truly want to uplift the profession, defend the workforce, and transform our systems, we must understand how therapists actually learn the work and why supervision must function as more than oversight.
Supervision is where clinical thinking develops.
It is where documentation becomes meaningful.
And it is where emerging clinicians begin to find their professional voice.
Therapist Development Is a Process, Not a Moment
Psychotherapy research consistently shows that therapists develop through identifiable stages as they move from novice to experienced clinician.
One of the most influential developmental frameworks comes from Skovholt and Rønnestad, whose research on therapist development describes a progression from early “lay helper” motivations to increasingly integrated professional identity. Their work highlights how clinicians evolve over time in areas such as confidence, flexibility, clinical judgment, and self-awareness.
The progression below illustrates how clinicians typically evolve from early technique-focused practice toward more flexible and integrated therapeutic work.
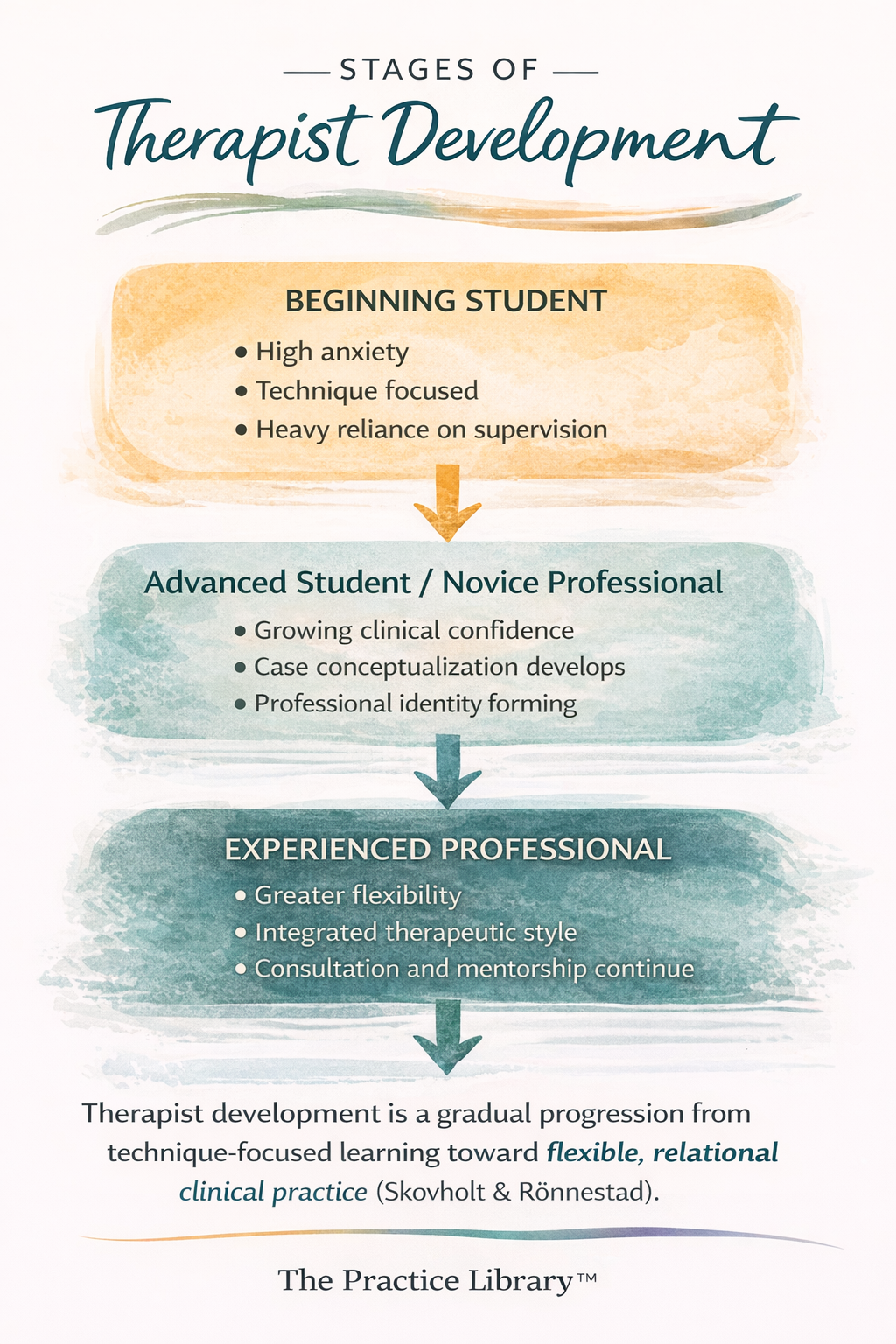
Therapist development stages illustrating the progression from early technique-focused practice toward greater clinical flexibility, confidence, and integration of professional identity.
Therapist development typically progresses from anxiety-driven technique focus toward increasing clinical flexibility, confidence, and integration of personal and professional identity.
Early in training, clinicians often rely heavily on empathy and personal experience as their primary frame of reference. As they enter graduate education and clinical placements, they begin to acquire theoretical frameworks and technical skills.
However, graduation does not mark the completion of clinical competence.
The early years of professional practice, particularly during associate licensure, are where therapists begin integrating:
theory and real-world clinical complexity
documentation and clinical reasoning
ethical decision-making and professional judgment
personal identity and professional role
Research suggests that the first five to six years of clinical work are particularly important for developing a stable professional identity and therapeutic style.
In other words, therapists are not fully formed at graduation.
They develop through experience, reflection, mentorship, and supervision.
Why Beginning Clinicians Often Feel Overwhelmed
Research on psychotherapy trainees consistently finds that beginning therapists experience high levels of anxiety in the therapy room.
Early clinicians often worry about:
saying the wrong thing
missing something important
choosing the wrong intervention
appearing incompetent to their supervisor
Because of this anxiety, beginners frequently focus intensely on technique and may believe there is a single “correct” way to conduct therapy.
Supervisors often observe that beginning therapists rely heavily on detailed process notes or transcripts during supervision. These notes function as an anxiety management strategy, allowing trainees to present every moment of a session in hopes that the supervisor will tell them what they should do next.
At this stage, trainees are often looking for certainty.
What they eventually learn is that psychotherapy rarely offers it.
Through repeated supervision conversations, clinicians gradually begin to internalize the supervisor’s clinical reasoning process. Over time, they shift from asking:
“What should I say?”
to asking:
“What is happening in the room, and what does this client need right now?”
This transition represents one of the most important developmental shifts in becoming a therapist.
Personal Motivation Is Not a Professional Weakness
Early in training, many students explain their interest in clinical work through personal experiences that shaped their values or drew them toward helping professions.
Sometimes this is misinterpreted as inappropriate self-disclosure or a lack of professional boundaries.
More often, however, it simply reflects a developmental reality.
Beginning clinicians interpret the work through the only frame of reference they currently possess - their own life experience.
Developmental models of therapist training show that personal meaning-making often precedes theoretical integration. Over time, clinicians learn to translate those personal motivations into professional frameworks and ethical practice.
When training environments shame or dismiss this early stage of development, students may internalize the message that they do not belong in the profession.
This is one of the ways imposter syndrome begins to take root.
Supportive supervision, on the other hand, helps trainees transform personal motivation into professional empathy, clinical curiosity, and ethical commitment.
The Associate Stage: Where Clinical Competence Deepens
The associate licensure period is often where clinicians develop the practical skills that sustain long-term professional practice.
By this stage, clinicians should be building competence in several key areas:
conducting comprehensive clinical assessments
developing case conceptualizations
writing defensible diagnostic justifications
developing and reviewing treatment plans
documenting progress notes that reflect clinical reasoning
conducting safety assessments and safety planning
collaborating with prescribers and medical providers
In many ways, this stage is where the principles discussed in my documentation articles - including Documentation Is Clinical Thinking Made Visible, The Golden Thread in Mental Health Documentation, and What Auditors Actually Look For in Behavioral Health Documentation - become real.
Graduate programs introduce documentation structures.
Supervision is where clinicians learn why those structures matter.
Documentation is not simply administrative work.
It is the written expression of clinical thinking.
Supervision helps clinicians learn how to connect assessment, diagnosis, treatment planning, and intervention into a coherent clinical narrative.
Moving From Rigidity to Clinical Flexibility
As clinicians gain experience, their relationship to theory often evolves.
Early in training, therapists may cling tightly to a specific modality or technique. This rigidity is often driven by anxiety and a desire to “do therapy correctly.”
Over time, clinicians gradually become more flexible.
Instead of asking whether they are following a particular model perfectly, they begin asking:
What is this client experiencing right now?
What interventions are most helpful in this moment?
How do my reactions in the room inform the work?
Experienced clinicians tend to integrate multiple theoretical perspectives and draw more intentionally on their own relational presence in the therapy process.
This shift from technique-driven practice to relational and conceptual flexibility is a hallmark of professional development.
Why Community Matters in Clinical Development
One of the greatest misconceptions about therapist training is that competence develops primarily through formal supervision.
In reality, clinicians develop through professional community.
Case consultation with colleagues, informal discussions about difficult sessions, mentorship relationships, and peer support all contribute to the development of clinical judgment.
These relationships also serve another essential function: containment.
Mental health clinicians routinely hold stories of trauma, grief, violence, and loss. Without opportunities to process the emotional impact of this work with trusted colleagues, clinicians can become isolated and overwhelmed.
Community is not a luxury in clinical work.
It is part of the infrastructure that sustains ethical practice.
In reality, most clinicians develop within a broader network of mentorship, consultation, peer discussion, and professional community.
I often think of this network as a supervision ecosystem that supports the development of clinical thinking and professional identity.
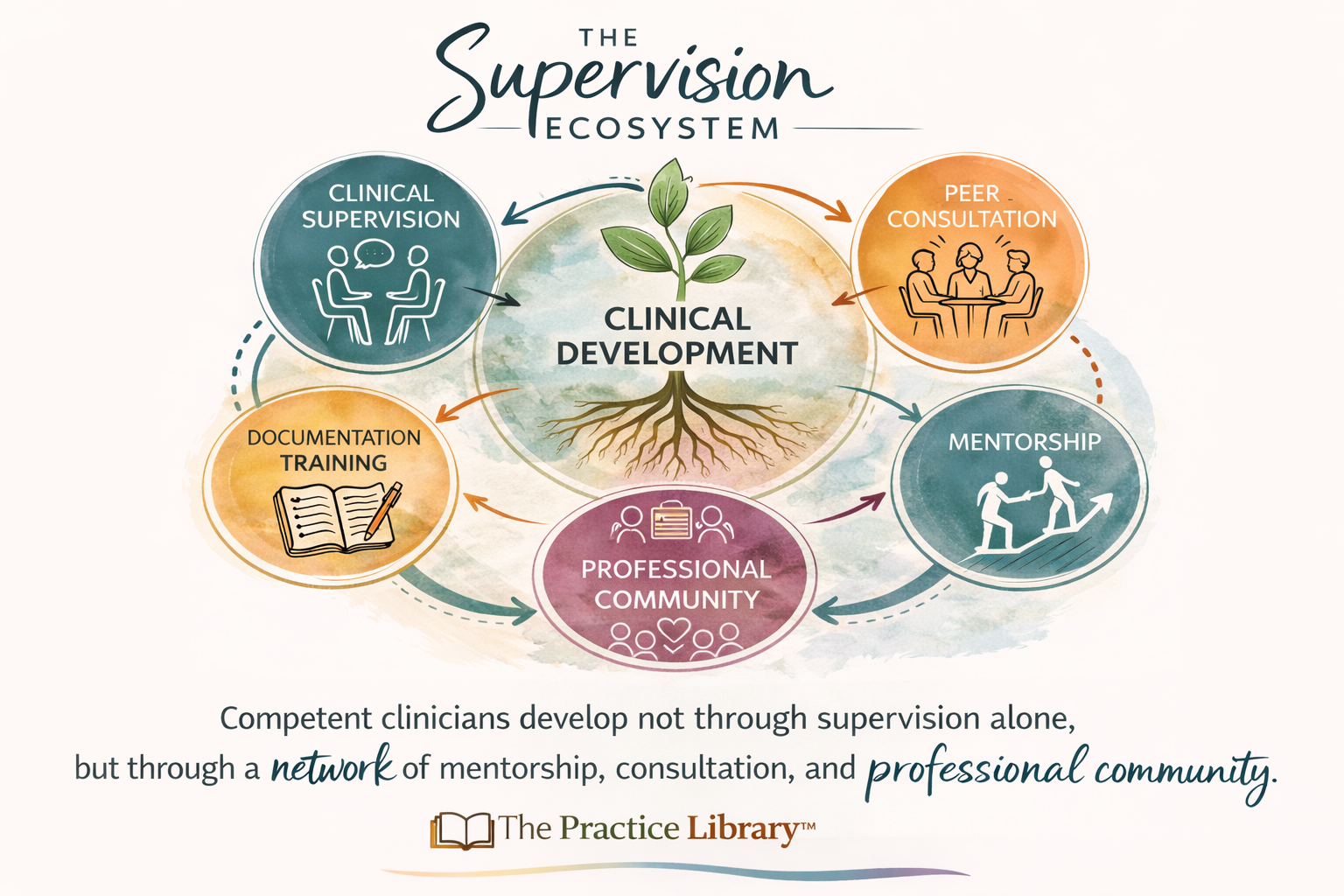
The Supervision Ecosystem Model
Developed by Shannon Webb, LICSW | SB Webb Counseling & Consulting | The Practice Library™
Building on supervision and developmental frameworks, this model illustrates how clinicians develop through interconnected systems of support.
Expanding Supervision Beyond a Single Relationship
Many clinicians benefit from seeking clinical consultation outside their primary supervision structure.
In this context, clinical consultation refers to case discussion, clinical reasoning, and professional reflection with experienced colleagues outside of one’s primary supervisory relationship.
Additional consultation can provide:
exposure to different theoretical perspectives
specialized expertise in particular clinical areas
broader professional mentorship
opportunities to strengthen documentation and case conceptualization skills
Building a network of consultation relationships early in one’s career helps clinicians develop both competence and resilience.
For some clinicians, this may include seeking additional supervision or consultation services focused on specific areas such as documentation, diagnostic formulation, or complex case conceptualization.
What matters most is not where consultation occurs, but that clinicians feel supported in continuing to develop their professional thinking.
Supervisor Development: Growth Happens on Both Sides of the Room
Just as clinicians develop over time, supervisors also move through identifiable stages of professional growth.
Early research on clinical supervision focused primarily on how supervisees develop. More recent models, including Loganbill, Hardy, and Delworth’s developmental supervision framework and the Integrated Developmental Model (IDM), recognize that supervisors themselves evolve as they gain experience, confidence, and professional perspective.
Supervision is therefore not a static skill set. It is a developmental practice.
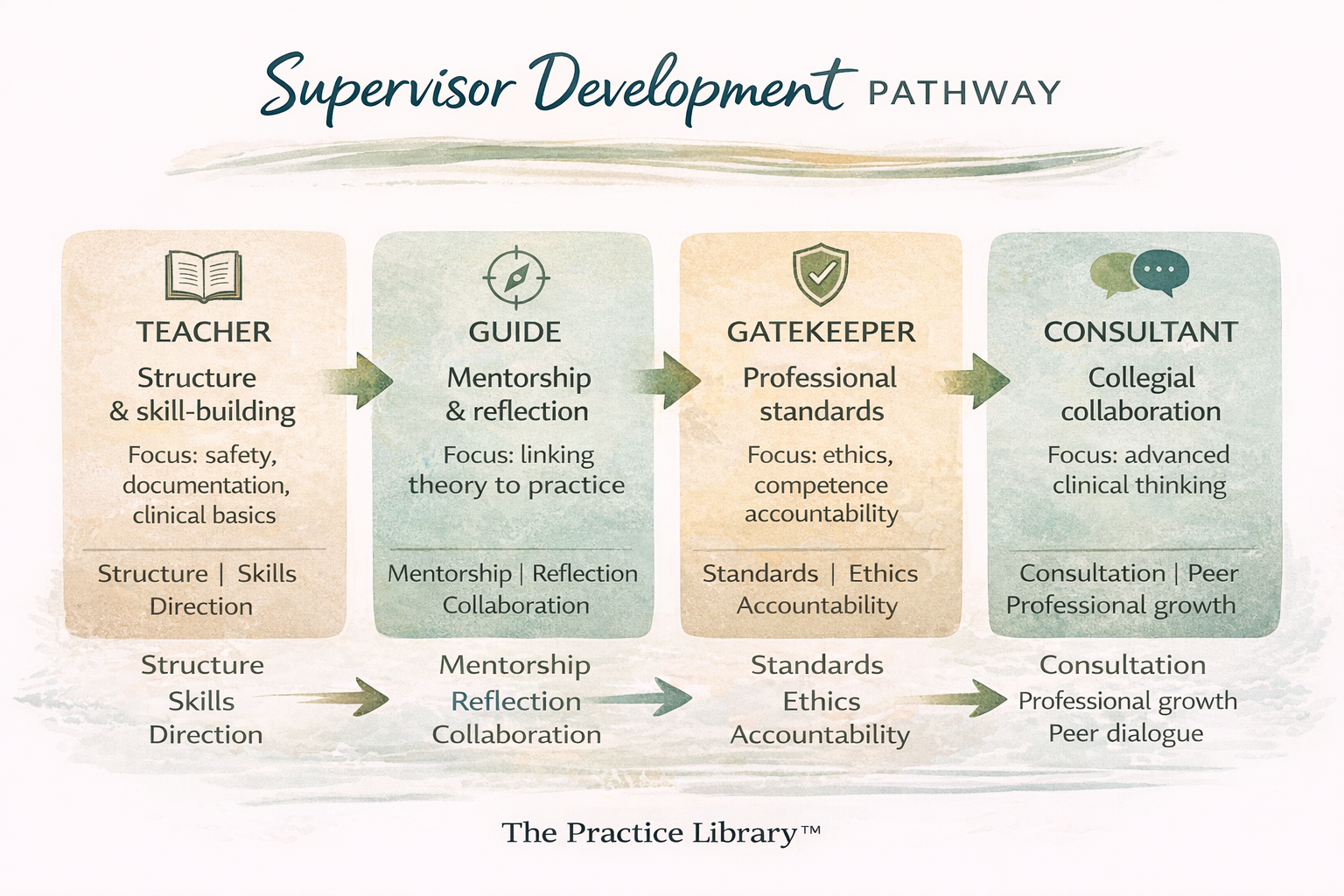
Many supervision scholars describe supervisor growth through a progression of roles that shift from directive teaching toward collaborative consultation.
Stage 1: The Teacher
Beginning supervisors often focus on structure, safety, and foundational skill development.
At this stage, supervisors may feel a strong responsibility to ensure that supervisees understand basic clinical expectations. Their supervisory style is often more directive as they provide guidance on topics such as:
documentation standards
ethical boundaries
clinical structure
basic intervention strategies
This structure is particularly helpful for early-career clinicians who may still be managing anxiety about conducting sessions and making clinical decisions.
Stage 2: The Guide
As supervisors gain experience, their role often shifts from direct instruction toward guided mentorship.
At this stage, supervision becomes more collaborative. Supervisors begin helping clinicians connect theoretical knowledge to real clinical situations, while encouraging greater independence in clinical decision-making.
The supervisory conversation increasingly focuses on:
case conceptualization
emotional responses to clinical work
professional identity development
Stage 3: The Gatekeeper
More experienced supervisors assume an important professional responsibility as gatekeepers for ethical and competent practice.
In this role, supervisors are comfortable addressing discrepancies between a clinician’s self-perception and their clinical performance. They help identify blind spots, challenge assumptions, and ensure that professional standards are maintained.
This stage may involve more direct conversations about:
ethical concerns
clinical competence
professional behavior
areas requiring further development
Gatekeeping is not about punishment. It is about protecting both clients and the integrity of the profession.
Stage 4: The Consultant
Over time, supervision often becomes more collegial.
At this stage, supervisors function more as consultants and mentors, particularly when working with experienced clinicians or advanced trainees. The supervisory relationship shifts toward collaborative exploration of complex cases, professional growth, and personal integration within the therapist role.
Rather than directing the work, the supervisor helps facilitate deeper reflection and high-level clinical thinking.
Supervision as a Parallel Developmental Process
One of the most important insights from supervision research is that supervisor development often mirrors clinician development.
Just as clinicians move from technique-driven practice toward flexible clinical reasoning, supervisors move from directive instruction toward collaborative consultation.
Effective supervision requires adapting one's approach based on the developmental needs of the supervisee. A beginning clinician may need clear structure and reassurance, while a more advanced clinician may benefit from reflective dialogue and conceptual challenge.
This dynamic process is sometimes described as a shift from “doing for” the supervisee toward “thinking with” the supervisee.
Recognizing supervision as a developmental process on both sides of the relationship helps create more responsive, thoughtful supervision environments.
For many supervisors, this realization also brings an important sense of perspective. Just as emerging clinicians benefit from patience, encouragement, and thoughtful guidance, emerging supervisors often rely on mentorship and collegial support as they develop their own supervisory voice.
Over time, many supervisors reflect on the grace that was extended to them during their own development, and recognize the importance of offering that same grace to the clinicians they now support.
It also reinforces an important truth about the profession:
We are all continuing to grow.
Matching Supervision to Developmental Need
Effective supervision is not only about the skill of the supervisor — it is also about the fit between the supervisor, the supervisee, and the stage of development both the clinician and the supervisor are navigating.
Beginning clinicians often benefit from supervisors who provide structure, clear expectations, and practical guidance around documentation, assessment, and clinical decision-making. At this stage, supervision may feel more instructional, helping clinicians translate academic training into real-world practice.
As clinicians gain experience, however, their needs often shift. Supervision becomes less about learning the mechanics of therapy and more about refining clinical judgment, exploring complex relational dynamics, and integrating multiple theoretical perspectives.
For more advanced clinicians, supervision often resembles consultation. The conversation may center on nuanced case formulation, ethical ambiguity, countertransference, or the broader professional challenges of sustaining a long-term career in behavioral health.
Because clinicians develop at different rates and bring different strengths to the work, no single supervisory style fits every clinician equally well. Thoughtful supervision requires attention not only to clinical content, but also to the developmental stage of the professional receiving it.
The Role of Peer Consultation
Formal supervision is only one part of the professional ecosystem that supports therapist development.
Peer consultation plays an equally important role.
As clinicians gain experience, many begin participating in peer consultation groups where colleagues discuss difficult cases, explore ethical dilemmas, and support one another in navigating the emotional demands of the work. These relationships can reduce professional isolation while strengthening clinical reasoning through collaborative reflection.
Peer consultation also provides a different kind of professional safety. While formal supervisors hold evaluative responsibilities, peer consultation relationships often create space for clinicians to openly examine uncertainty, mistakes, and learning edges without the pressure of formal evaluation.
In this way, peer consultation functions as a parallel layer of professional containment that complements formal supervision.
In practice, however, access to peer consultation is not always straightforward. Clinicians often work full clinical schedules that do not easily align with colleagues’ availability, making it surprisingly difficult to create consistent consultation spaces. It is common for therapists to discover that their closest professional peers work entirely different hours, serve different populations, or practice in different systems of care.
Practice setting can also influence how easily clinicians access collaborative support. Therapists working within group practices, hospitals, or agency settings often benefit from built-in opportunities for consultation through treatment teams, case staffing meetings, or informal conversations with colleagues. These environments can provide valuable opportunities to compare perspectives, refine clinical reasoning, and observe how other clinicians approach complex cases.
Clinicians working in private practice may experience greater professional autonomy, but they also often need to intentionally create their own consultation networks. Many private practitioners rely on a single supervisor while paying for supervision out of pocket, and without an organizational structure around them, opportunities for spontaneous case consultation may be limited.
For newer clinicians especially, having access to multiple perspectives can be invaluable. Collaborative environments allow clinicians to “ping ideas” off colleagues, explore alternative conceptualizations, and consider how clinicians with different specialties or theoretical orientations might approach the same case.
This is not about one setting being better than another. Rather, it highlights the importance of actively cultivating professional community, particularly in the early years of practice. Whether through formal consultation groups, mentorship relationships, supervision networks, or interdisciplinary collaboration, clinicians benefit when they are not navigating complex clinical work entirely on their own.
Peer consultation, like supervision, helps sustain both clinical judgment and professional resilience. Together, these relationships form part of the broader ecosystem that allows therapists to continue developing throughout their careers.
Supervision Is a Professional Infrastructure
When we step back, it becomes clear that supervision is not simply an individual relationship. It is part of the professional infrastructure that sustains ethical clinical practice.
Administrative supervision helps ensure that organizations operate safely and responsibly. Clinical supervision supports the development of therapeutic skill, ethical judgment, and professional accountability. Consultation and peer collaboration provide additional perspectives that help clinicians navigate the complexity of real-world clinical work.
Together, these layers form the professional scaffolding that allows therapists to grow over time while maintaining accountability to the clients they serve.
Over the course of a career, the nature of supervision often changes. Early-career clinicians frequently need structured guidance around documentation, assessment, ethical decision-making, and clinical intervention. At later stages of professional development, however, supervision may become less about instruction and more about consultation, reflection, and professional support.
Seasoned clinicians often arrive in supervision with years of clinical experience behind them. They have already mastered many of the fundamental competencies of practice. What they may need instead is space to think through complex cases, to process the cumulative emotional weight of the work, or to reflect on how to sustain themselves in a profession that frequently exposes clinicians to trauma, loss, and systemic strain.
For supervisors, this requires an important kind of professional flexibility. Effective supervisors learn to move fluidly between roles depending on the needs of the clinician in front of them. At times the supervisor may function as a teacher, offering structure and foundational guidance. At other times the role may shift toward mentorship, ethical oversight, or collegial consultation.
Even within a single supervisory relationship, these roles may shift from week to week. A clinician who generally operates with significant autonomy may encounter a particularly complex case that requires more structured guidance. Another clinician may be navigating burnout or professional transition and benefit from reflective mentorship rather than technical instruction.
Supervision therefore requires supervisors to develop awareness not only of their supervisees’ developmental stage, but also of their own supervisory stance. Knowing when to teach, when to guide, when to challenge, and when to collaborate is part of the craft of supervision itself.
Equally important is the responsibility to cultivate the next generation of supervisors. As experienced clinicians move through their own professional development, many begin mentoring newer clinicians who will eventually take on supervisory roles themselves. Supporting emerging supervisors in learning the ethical, legal, and relational dimensions of supervision is essential for sustaining the profession over time.
Supervision, in this sense, is not only about supporting individual clinicians. It is about strengthening the professional ecosystem that will support future generations of practitioners.
Many clinicians strengthen their professional development by engaging in supervision mentorship, peer consultation groups, or structured clinical consultation relationships throughout their careers.
Transforming the Culture of Supervision
If we want to uplift the profession, we must support the clinicians doing the work.
If we want to defend the workforce, we must recognize the developmental challenges faced by early-career therapists and the cumulative demands faced by experienced clinicians.
And if we truly want to transform our systems, we must treat supervision as more than a regulatory requirement.
Supervision is where clinicians learn to think.
It is where theory becomes practice.
Where documentation becomes meaningful.
Where professional identity begins to form.
It is also where clinicians reflect on the emotional impact of the work, reconnect with professional purpose, and sustain the resilience required to continue practicing ethically over time.
Clinical competence does not develop in isolation.
It develops through supervision, consultation, mentorship, and professional community.
And when supervision functions as a thoughtful, responsive, and collaborative process, it becomes one of the most powerful ways we can strengthen both the profession and the people who carry its work forward.
References
Bernard, J. M., & Goodyear, R. K. (2019). Fundamentals of clinical supervision (6th ed.). Pearson.
Hill, C. E., & Knox, S. (2013). Training and supervision in psychotherapy. In M. J. Lambert (Ed.), Bergin and Garfield's handbook of psychotherapy and behavior change (6th ed.). Wiley.
Loganbill, C., Hardy, E., & Delworth, U. (1982). Supervision: A conceptual model. The Counseling Psychologist, 10(1), 3–42.
Rønnestad, M. H., & Skovholt, T. M. (2013). The developing practitioner: Growth and stagnation of therapists and counselors. Routledge.
Skovholt, T. M., & Rønnestad, M. H. (1992). The evolving professional self: Stages and themes in therapist and counselor development. Wiley.
Skovholt, T. M., & Rønnestad, M. H. (2003). Struggles of the novice counselor and therapist. Journal of Career Development, 30(1), 45–58.
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors and therapists (3rd ed.). Routledge.
SB Webb Counseling & Consulting PLLC | The Practice Library™
Clinical supervision and consultation with integrity, structure, and relational mentorship.
sbwebbcounselingconsulting.org