

Becoming an Approved Supervisor in Washington: Beyond the 25-Hour Requirement
Understanding the “supervision of supervision” requirement following the initial 15 hours of training.
SB Webb Counseling & Consulting PLLC | The Practice Library™
sbwebbcounselingconsulting.org
If you’re a licensed clinician in Washington State thinking about becoming an approved supervisor, you’ve likely come across the requirement of:
25 hours of experience in the supervision of clinical practice.
This requirement is often referred to as “supervision of supervision,” and it reflects the expectation that supervisors develop competency in overseeing clinical work — not just providing it.
On paper, it sounds straightforward.
But in practice, this is one of the most misunderstood, and most consequential, parts of becoming a supervisor, particularly for clinicians who have not yet had direct supervisory experience
Over the course of my work across community mental health, integrated care, and private practice, I’ve supported clinicians at every stage - from intern, to associate, to full licensure, to stepping into supervision and leadership roles of their own.
And what I’ve seen consistently is this:
The 25-hour requirement isn’t just about completing hours.
It’s about developing the capacity to hold responsibility for another clinician’s work; clinically, ethically, and systemically.
Let’s break down what that actually means.
Becoming an Approved Supervisor in Washington isn’t just about completing 25 hours. It’s about developing the capacity to hold responsibility for another clinician’s work—clinically, ethically, and systemically. Many clinicians are prepared clinically, but not always prepared for the systems that shape practice. This is where supervision becomes more complex—and more important.
The Requirement (WAC 246-809-134 & 246-809-334)
In Washington State, becoming an approved clinical supervisor for LMHCs, LMFTs, or LICSWs is clearly defined in WAC 246-809-134 and WAC 246-809-334.
At a minimum, supervisors must complete:
15 hours of supervision training
25 hours of experience in the supervision of clinical practice
In addition, supervisors must:
Hold an active, unrestricted license in good standing for at least two years
Provide a formal declaration of qualification prior to supervising
Demonstrate working knowledge of:
ethical standards
documentation and recordkeeping
financial and billing practices
clinical oversight
continuity of care and coverage planning
There is also an established exception:
Clinicians who are AAMFT Approved Supervisors are considered to have met these requirements.
Supervisor Requirements: Washington vs. New York vs. Texas - At A Glance
One of the things that becomes clear when looking at supervision requirements more closely is that they are not standardized across states.
While the core responsibilities of supervision remain consistent—clinical oversight, ethical accountability, and professional development—the structure and expectations can vary significantly depending on the regulatory environment.
The comparison below highlights how Washington State aligns with, and differs from, other states in key areas of supervision training, experience, and oversight.
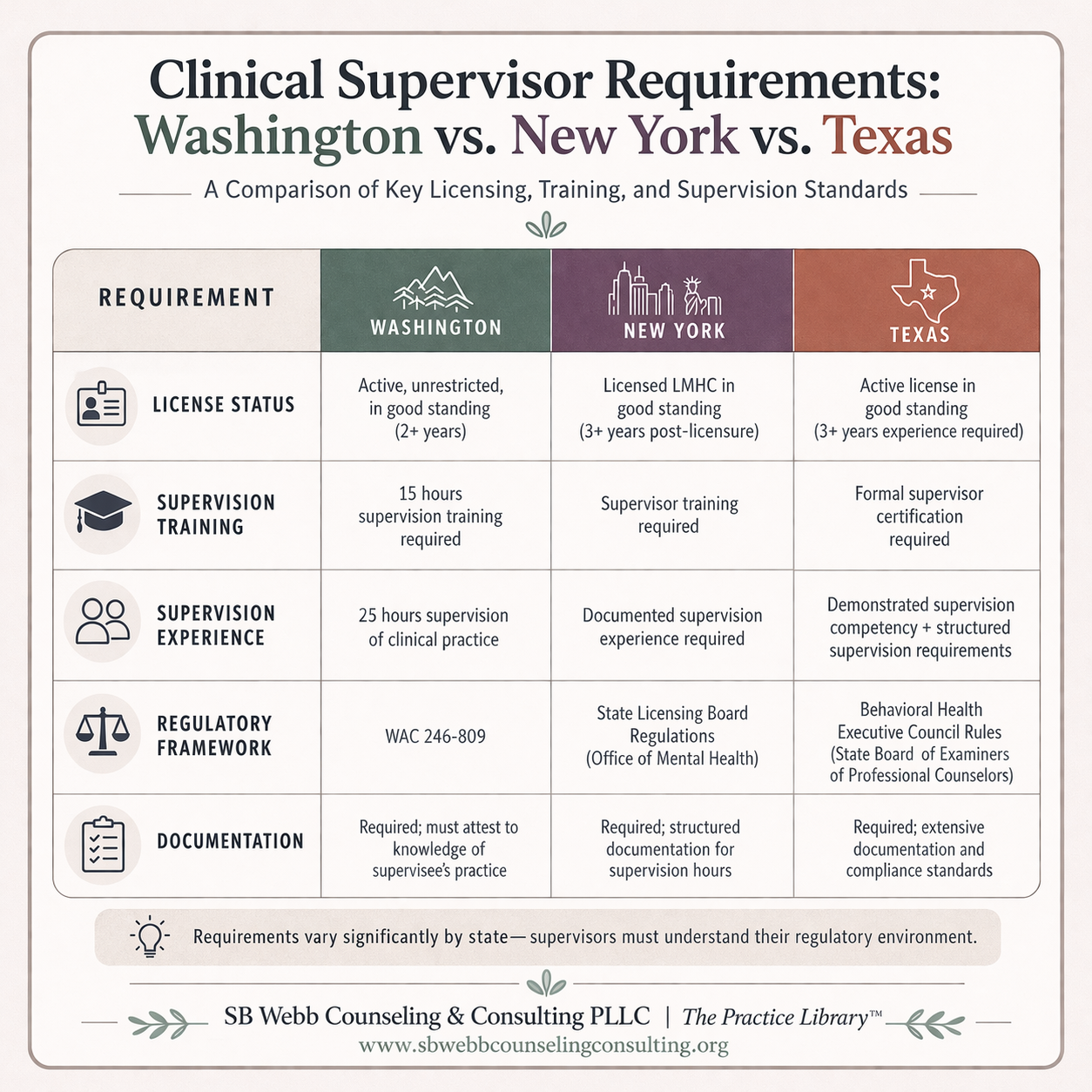
This graphic compares clinical supervisor requirements in Washington State, New York, and Texas, including supervision training hours, experience requirements, documentation standards, and regulatory frameworks. It demonstrates how supervision expectations vary across states and underscores the importance of systems knowledge in clinical supervision.
Requirements vary by state and discipline, but the core expectation remains consistent: supervisors must be prepared to take responsibility for the clinical, ethical, and professional development of the supervisee.
WHAT THE 15 HOURS SHOULD ACTUALLY COVER
Not all 15-hour supervision trainings are created equal.
Based on best practice standards and formal supervision training models, effective supervision training should include:
Legal and ethical responsibilities of supervision
Understanding liability (direct and vicarious)
Development of supervision agreements and contracts
Models and theories of supervision
Documentation standards and audit readiness
Managing boundaries and dual relationships
Cultural awareness and cross-cultural supervision
Risk management, including safety and mandated reporting
Navigating complex clinical scenarios (e.g., lethality, subpoenas)
These areas are not just theoretical — they directly impact how supervisors make decisions and manage risk in real-world practice.
Supervision carries both clinical and legal responsibility, including potential liability for supervisee actions.
Where This Gets More Complex in Practice
While the WAC language is relatively straightforward, the application of these requirements is where many clinicians get stuck.
Having sat through state trainings, reviewed the WAC in practice settings, and supported clinicians as they move from associate to fully licensed, and eventually into supervisory roles themselves, one thing becomes clear:
The state is not just asking whether you’ve completed hours.
It is asking whether you have developed the competence to oversee clinical practice in real-world systems.
This includes not only clinical guidance, but also:
how care is documented
how services are billed
how ethical decisions are made in context
and how clinicians function within their specific practice environment
This is the level of understanding that supervision of supervision is intended to build.
What Many People Miss
The requirement isn’t just about logging hours.
It’s about demonstrating that you can hold responsibility for another clinician’s work in real-world practice.
And that’s where things often become more complex than expected.
“Supervision is not just about guidance — it is about accountability”
In my experience supporting clinicians across settings — from early training through licensure and into supervision — the transition into this level of responsibility is where many people feel the shift.
Because supervision at this level requires you to:
Hold clinical and ethical responsibility for another provider’s care
Navigate complexity in documentation, billing, and decision-making
Understand how systems impact clinical practice — not just the therapy itself
Support clinician growth while maintaining accountability to client safety
This is not just a developmental step — it is a shift in role.
And it’s often where gaps in preparation become most visible.
Supervision doesn’t happen in isolation.
It happens inside systems that directly impact care, compliance, and sustainability.
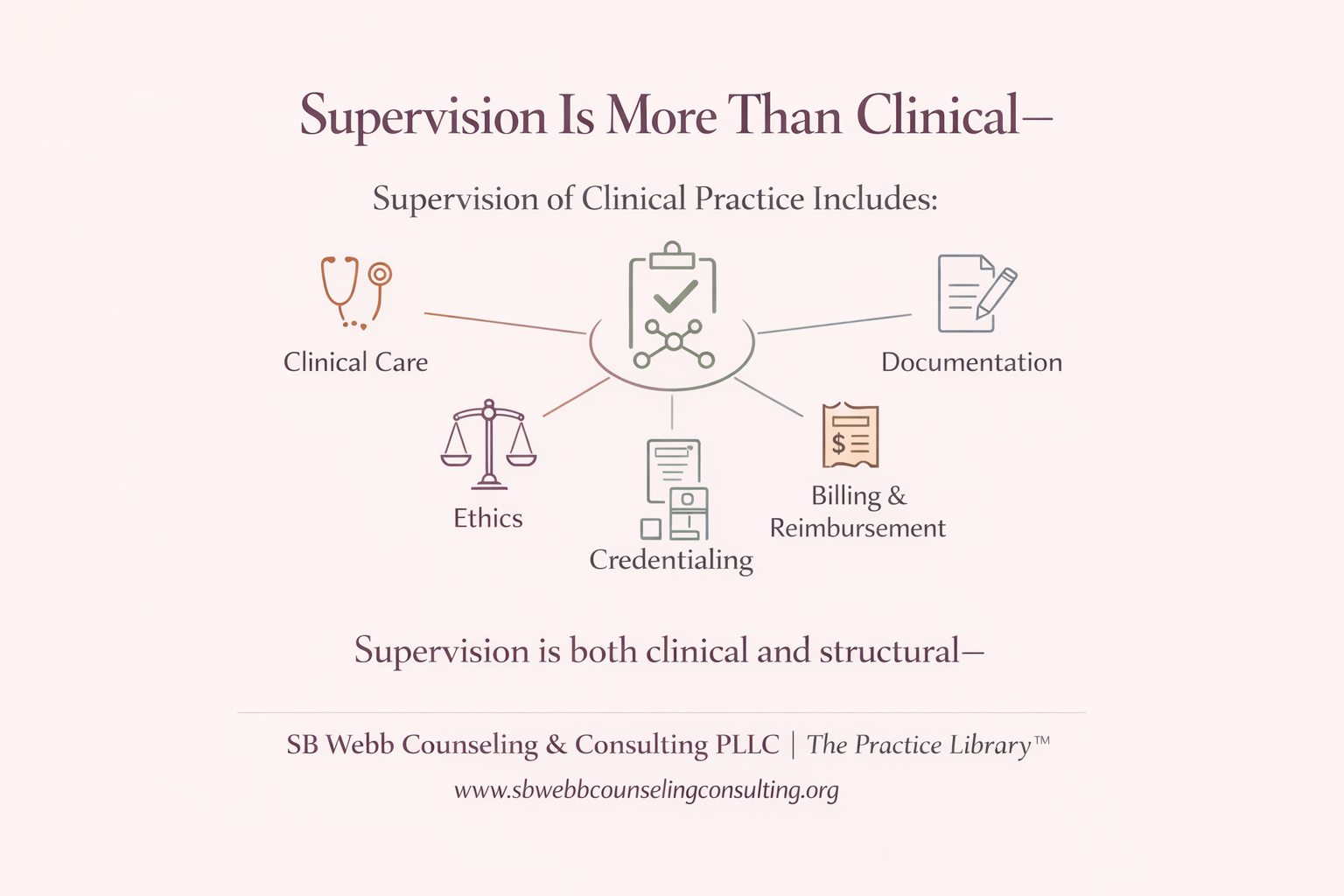
Supervision is often understood as clinical guidance—but in practice, it extends far beyond that. Documentation, billing, credentialing, and compliance all shape how care is delivered. Strong supervision requires understanding both clinical work and the systems that sustain it.
This is why the 25-hour requirement is not simply a threshold — it is a structured process of developing competency in supervision of supervision.
Supervision Isn’t Just Clinical — It’s Structural
Many clinicians feel confident in their clinical skills before becoming supervisors.
But supervision requires an additional layer:
Understanding licensure pathways
Knowing how documentation holds legal weight
Navigating insurance, billing, and compliance systems
Supporting clinicians across different practice settings
For example:
If your supervisee is in private practice or billing insurance, you need to understand things like:
NPI vs. NPPES
CAQH credentialing
OneHealthPort access
Taxonomy alignment and claim submission
Because these aren’t “admin tasks” they directly impact:
reimbursement
ethical practice
continuity of care
Even something as simple as using the wrong taxonomy can lead to claim denials or compliance issues.
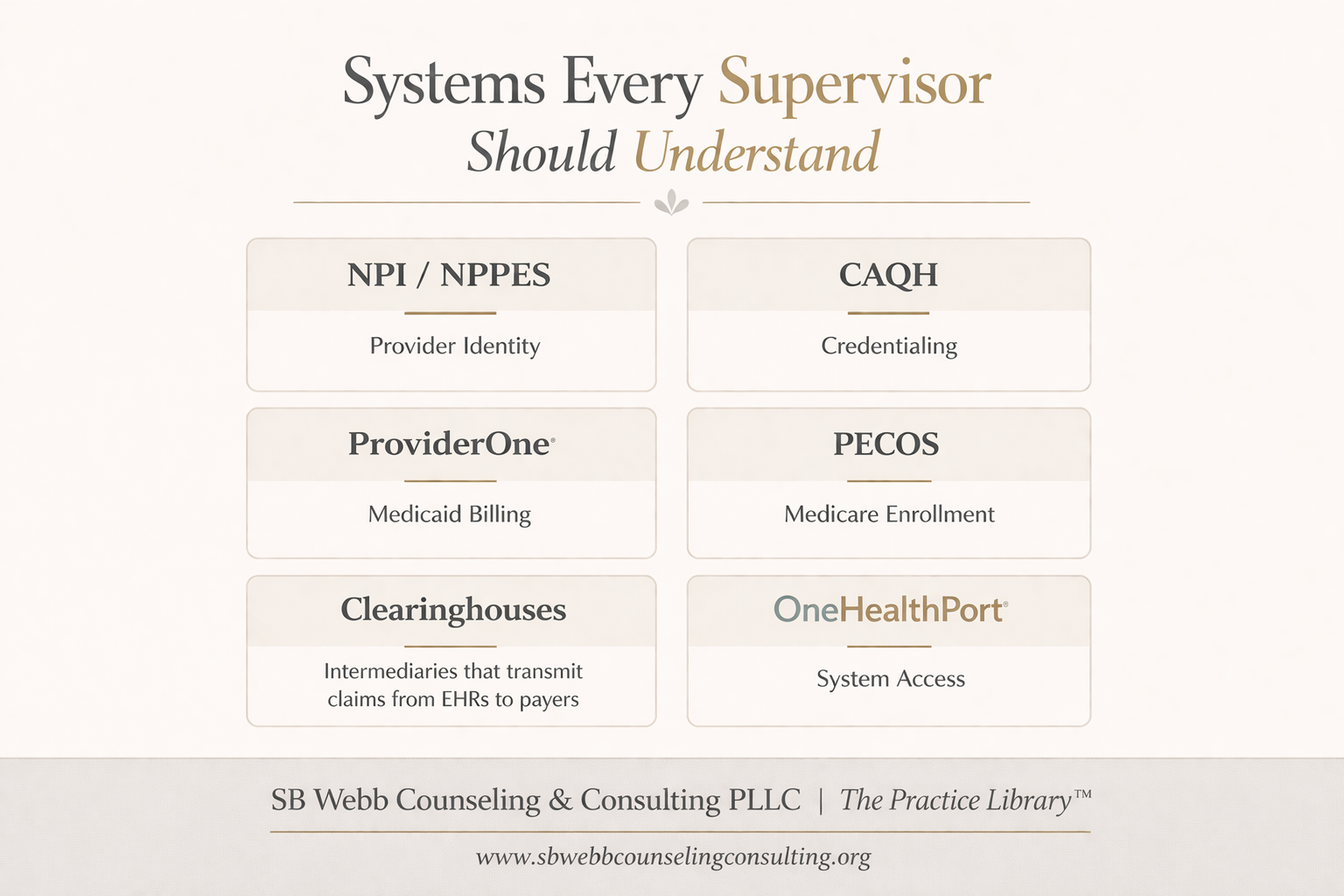
The “Alphabet Soup” — and the Systems Supervisors Actually Need to Understand
If you’re supervising clinicians today — whether they are LMHCs, LMFTs, LICSWs, or other behavioral health providers, you are not just supporting clinical work.
You are supporting how that work exists within healthcare systems, payer structures, and regulatory environments.
That means having working knowledge of more than just a few acronyms.
It means understanding the full landscape of how clinicians are:
identified
credentialed
enrolled
and ultimately paid
If you’re supervising clinicians, you’re not just supporting therapy.
You’re supporting how that therapy is documented, credentialed, billed, and sustained.
Supervisors don’t need to manage every system—but they do need to understand how those systems impact care. Credentialing delays, billing errors, and access issues can directly affect reimbursement, compliance, and continuity of care. This is part of supervision—not separate from it.
Core Identity & Enrollment Systems
NPI (National Provider Identifier)
A unique 10-digit identifier required for all HIPAA-covered transactionsNPPES (National Plan & Provider Enumeration System)
The federal system where providers apply for and maintain their NPI
This is foundational and without it billing and credentialing cannot happen
Credentialing & Insurance Paneling
CAQH ProView
The centralized credentialing database used by most commercial insurers
(Aetna, Premera, Regence, etc.)Insurance Paneling Processes
Vary by payer and may include:direct enrollment
group-based credentialing
third-party platforms (Headway, Alma, Grow)
Supervisors should understand how clinicians become paneled and the timelines, barriers, and implications of each pathway
Government Payer Systems
ProviderOne (Washington Medicaid)
Required for billing Apple Health / Medicaid in WAOneHealthPort (WA-specific)
Secure single sign-on used to access multiple payer portals, including Medicaid systemsPECOS (Medicare Enrollment System)
Required for clinicians who plan to bill Medicare
These systems introduce additional compliance, enrollment, and documentation expectations that directly impact practice
Claims & Billing Infrastructure
Clearinghouses
Intermediaries that transmit claims from EHRs to payersEHR / Practice Management Systems
(e.g., TherapyNotes, SimplePractice)
Used for documentation, billing, and recordkeeping. Depending on the platform, these systems may also support credentialing processes, insurance claim submission, and direct integration with payer systems
These systems aren’t random—they follow a sequence.
Understanding the flow helps supervisors identify where things break down.
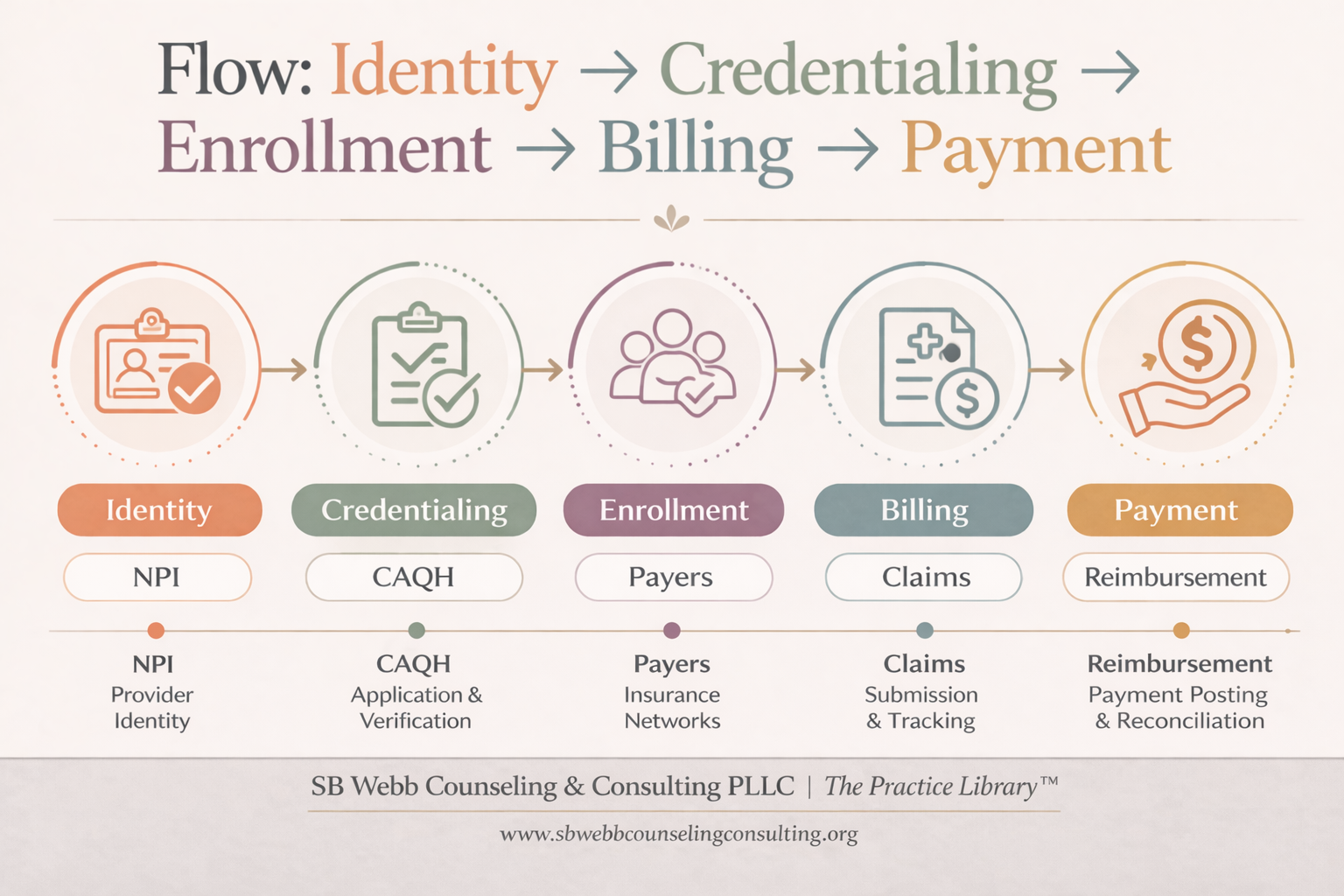
Clinical work exists within a sequence of systems: identity → credentialing → enrollment → billing → payment. When supervisors understand this flow, they can identify breakdowns earlier—and support clinicians more effectively. This is where systems knowledge becomes clinical impact.
Supervisors are not responsible for managing these systems, but they do need to understand how breakdowns within them can impact clinical care, reimbursement, and compliance.
The level of support these systems provide can also shape how a clinician practices and what is required of a supervisor in providing effective oversight.
A Note on Ownership of Your Professional Identity
One important, and often overlooked, part of this conversation is access.
In some settings, associates may not have direct access to their own:
NPI / NPPES profile
CAQH account
credentialing applications
payer enrollments
These may be managed at the agency or group level.
While this can streamline onboarding in some environments, it can also create gaps in understanding and, at times, limit a clinician’s ability to navigate their own professional identity across settings.
Over time, clinicians benefit from understanding:
where their information is housed
how their credentials are being used
and how to access or manage these systems independently
This becomes especially important when transitioning between roles, settings, or into private practice.
Here’s something many clinicians don’t realize until much later:
They may not actually have access to their own professional systems.
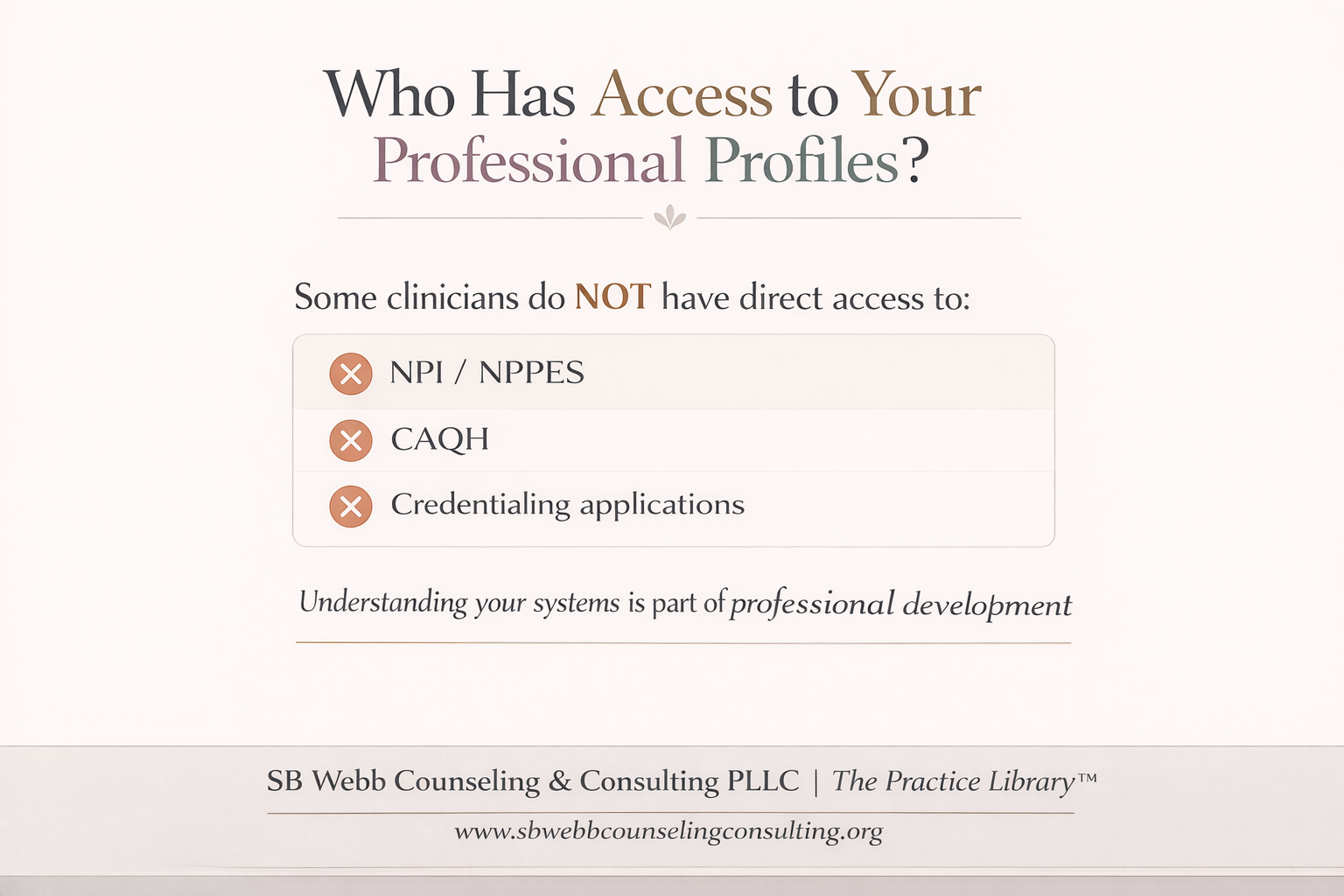
Here’s something many clinicians don’t realize: They may not have direct access to their own professional profiles. NPI, CAQH, credentialing applications—these are sometimes managed at the agency or group level. Understanding where your information lives is part of professional development—and long-term mobility.
Supervision can play an important role here, not by managing these systems for the clinician, but by helping them understand how they work and what questions to ask.
“The level of access shapes the level of accountability”
Why This Matters for the 25-Hour Requirement
Because supervision of clinical practice doesn’t happen in a vacuum.
It happens within systems and within the realities of different practice settings.
True supervision experience includes:
Reviewing documentation with an understanding of billing and audit risk
Supporting clinicians through credentialing and enrollment decisions
Recognizing how payer requirements shape clinical practice
Identifying issues before they result in claim denials, audits, or ethical concerns
At the same time, the level of access and oversight a supervisor has can vary significantly depending on the setting.
In agency or group practice environments, supervisors may not have direct access to clinical documentation or billing systems. In these cases, supervision often relies on:
case consultation and staffing
clinical discussion and review of decision-making
collateral information about documentation and care processes
This is one of the reasons it is important to clearly distinguish between:
Immediate or direct supervision of clinical work
Supervision of experience hours
Oversight of direct counseling hours
Each carries different expectations for access, responsibility, and depth of review.
As a result, supervision may require additional dialogue, clarification, and intentional structure to ensure appropriate oversight — even when full access to systems or records is not available.
Without this level of awareness, supervision can remain:
supportive, but not fully accountable
clinically strong, but systemically limited
And Washington State is clear:
Approved supervisors must have thorough knowledge of the supervisee’s practice and not just their clinical work, but how that work is delivered, documented, and sustained.
The structure of supervision matters, because the level of access directly shapes the level of accountability including understanding what auditors actually look for in behavioral health documentation.
How Clinical Work Becomes Sustainable Practice
Supervisors are often expected to support clinicians not only in clinical care, but in understanding how that care is sustained in practice.
Depending on the setting, this may include navigating:
commercial insurance paneling
Medicaid enrollment (ProviderOne in Washington)
Medicare enrollment (PECOS)
third-party platforms that support credentialing and billing
These processes are not separate from clinical work, they directly shape:
who a clinician can serve
how services are delivered
whether care is reimbursed and sustained over time
This is where supervision extends beyond clinical guidance.
Supervisors who are unfamiliar with these systems may unintentionally limit a supervisee’s ability to practice independently, transition between settings, or build a sustainable caseload.
In contrast, supervisors who understand these structures are better positioned to support clinicians in making informed decisions about their practice setting, payer mix, and long-term development.
A Shift in How We Think About Supervision
The 25-hour requirement isn’t just a box to check.
It’s there for a reason.
Over time, what I’ve come to understand — both through my own work and supporting others into supervisory roles — is that this requirement is really about readiness.
Readiness to move from being responsible for your own clinical work…
to being responsible for someone else’s.
That shift matters.
Because strong supervisors are not just good therapists. They are people who can hold ethical complexity, understand how systems shape care, and stay grounded in accountability — even when things are unclear or evolving.
Supervision Looks Different Depending on Where Your Clinician Works
Supervision doesn’t look the same in every setting.
The structure around a clinician changes what supervision needs to provide.
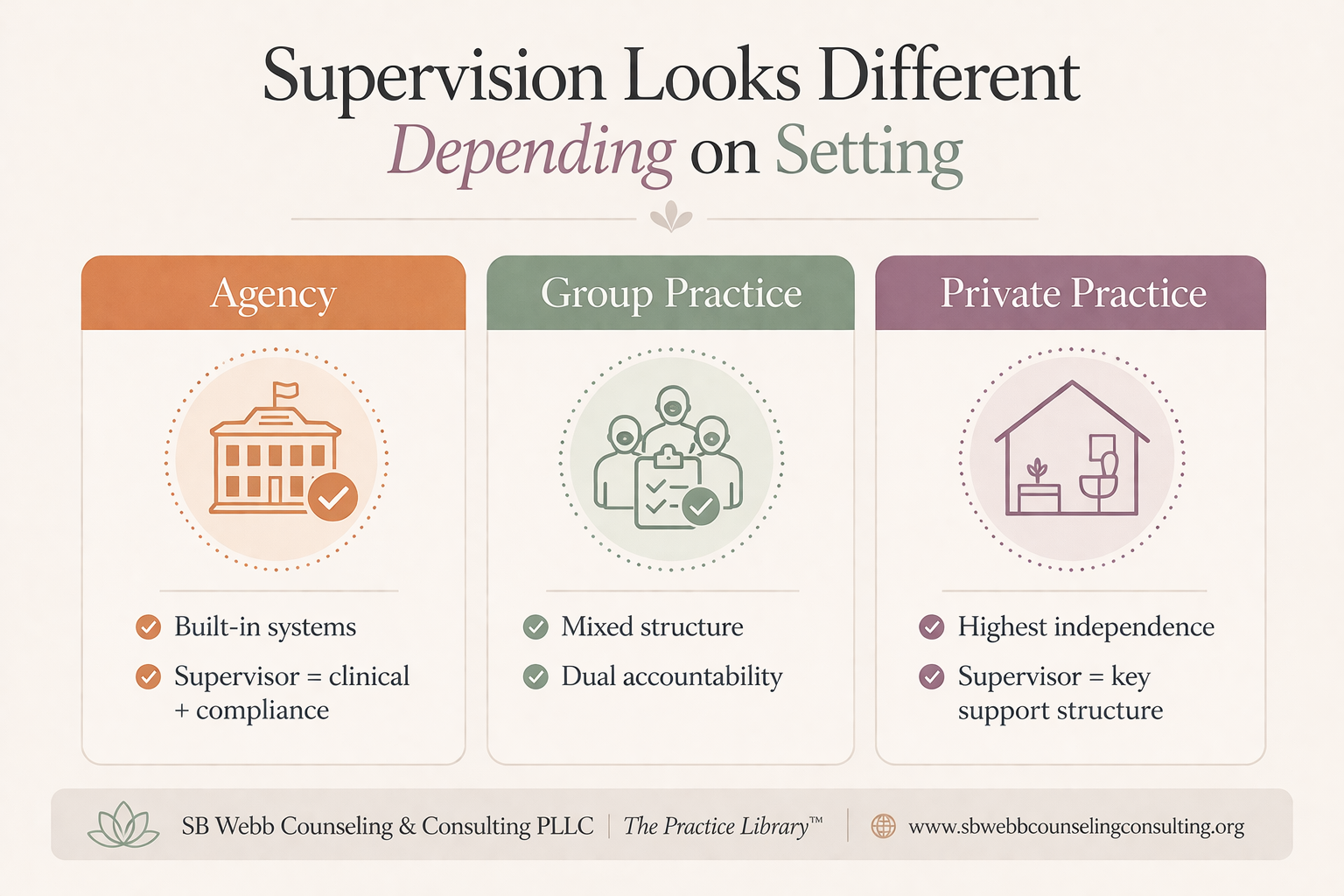
Supervision is not one-size-fits-all. The needs of supervision shift depending on whether a clinician is in agency, group practice, or private practice. Structure, access, and accountability all change depending on the setting. Effective supervisors adjust accordingly.
One of the things that often gets overlooked is that supervision is not one-size-fits-all.
It changes depending on where and how your supervisee is practicing.
In agency or community mental health settings, there is often already a structure in place — billing systems, credentialing support, compliance processes. In those environments, supervision may lean more heavily into clinical quality, documentation, and risk management within an established system.
In group practice, things can be more variable. There may be some infrastructure, but not always consistency. Supervisees might be navigating expectations from both the practice and their supervisor. In those cases, supervision often includes helping them make sense of contracts, documentation expectations across different payors, and how to hold responsibility within more than one structure.
Private practice is where this becomes even more nuanced.
When someone is practicing independently, supervision often becomes one of the primary places where clinical, ethical, and sometimes even structural questions get worked through. That can include decisions about credentialing, how they are billing, how they are documenting, and how they are thinking about risk and compliance in a setting where there may not be built-in oversight.
In those situations, supervision isn’t just about supporting clinical work — it becomes part of the framework that helps hold the practice itself.
Why the “Supervision Ecosystem” Matters
While much of this conversation has focused on regulatory requirements and systems, it’s also important to recognize that clinical development does not happen through supervision alone.
As explored further in The Supervision Ecosystem, clinical development does not happen through supervision alone, it exists within a broader professional ecosystem that includes mentorship, consultation, training, and community.
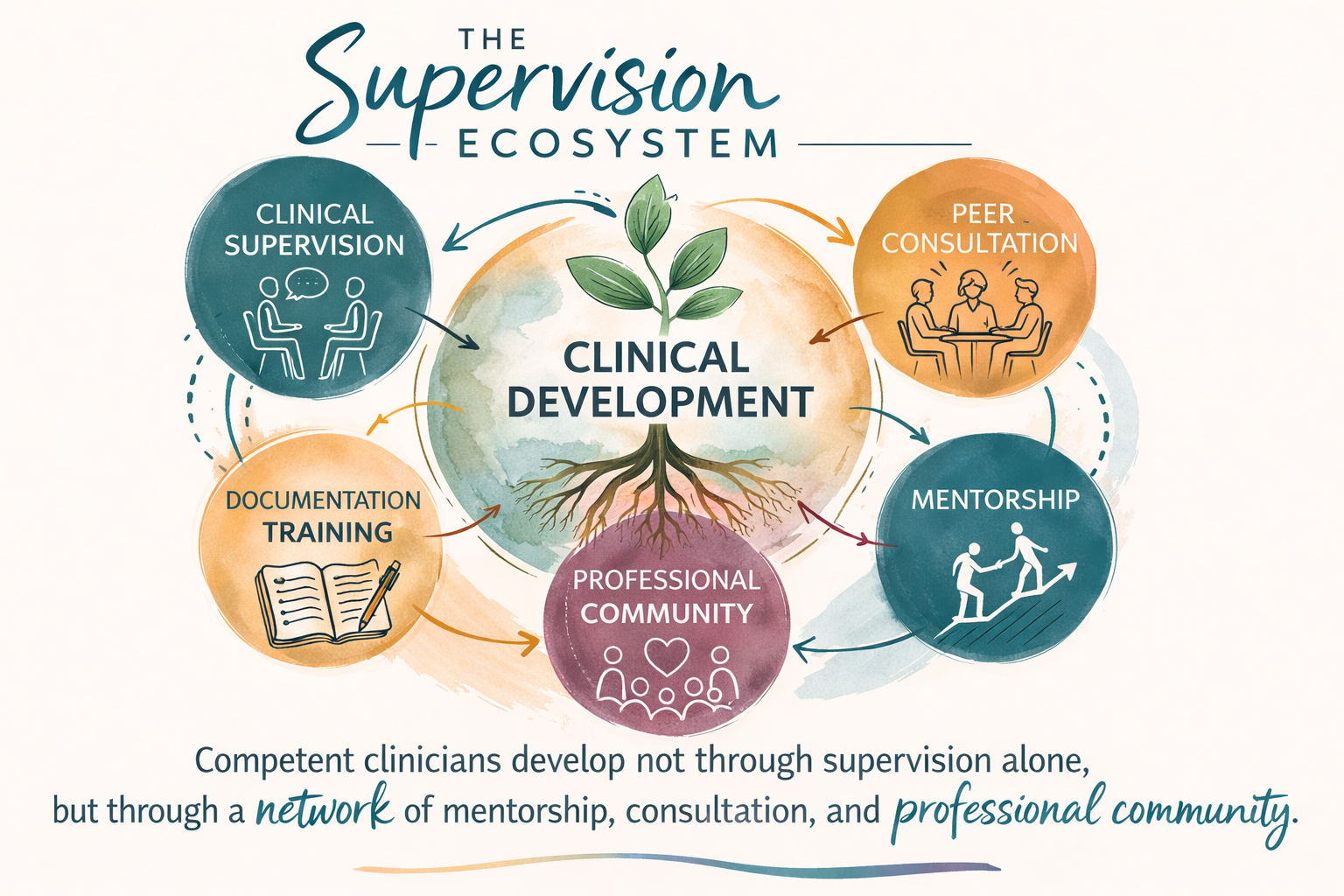
This graphic illustrates the broader supervision ecosystem, highlighting how clinical supervision interacts with mentorship, peer consultation, documentation training, and professional community to support clinician development.
Supervision doesn’t happen in isolation.
It sits within a broader ecosystem — one that includes regulatory requirements, payer systems, practice settings, clinical complexity, and ethical responsibility.
But it also exists within something less visible — the internal world of the clinician.
The emotional weight they carry.
The complexity they hold.
The responsibility of sitting with other people’s pain, trauma, and uncertainty — day after day.
As explored in Uplift the Workforce: Why Clinical Supervision Is More Than Oversight, supervision is not simply a requirement — it is one of the primary places where clinicians develop professional identity, clinical judgment, and ethical grounding within the realities of the work.
At the same time, clinicians are not meant to hold this work alone. As discussed in Who Holds the Helpers?, the absence of meaningful support structures can lead to burnout, isolation, and increased risk within the profession itself.
This is where supervision intersects not only with competence, but with sustainability.
Over time, what becomes clear is that these elements do not operate separately — they interact, shaping how clinicians practice both externally and internally.
Effective supervisors learn how to hold all of that in view.
Not perfectly, and not all at once — but with enough awareness to understand how decisions in one area can impact another.
This includes recognizing that what is often labeled as “imposter syndrome” may reflect something deeper — a lack of containment, support, and professional community (see Beyond Imposter Syndrome: Supervision, Community, and the Workforce We’re Building).
Because ultimately, supervision is not just about supporting the clinician.
It is about protecting the client, supporting the clinician as a whole person, and maintaining the integrity of the system of care they are working within.
It is also about recognizing that clinicians are not just providers of care — they are people who carry, process, and make meaning of human experience in real time.
And that requires not only skill and knowledge, but space, support, and accountability.
Supervision Is Also About Access
There’s also a very practical side to this.
This isn’t just about understanding systems for the sake of knowledge.
It directly impacts how quickly—and how sustainably—a clinician can practice.
When systems are well understood: ✔ Faster credentialing ✔ Fewer billing issues ✔ More consistent care
When they’re not: ✖ Delays ✖ Denials ✖ Disruptions in care
This isn’t administrative—it directly impacts clinical work.
When supervisors understand how systems work, it can make a real difference in how quickly and sustainably a clinician is able to practice.
Credentialing moves more smoothly.
Billing issues are caught earlier.
Services are more consistent for clients.
When those systems aren’t well understood, the impact shows up differently.
Delays in credentialing.
Denied claims.
Interruptions in care.
And often, clinicians feeling stuck or unsure of how to move forward.
This is part of the work, too.
“Supervision doesn’t just support clinicians — it helps sustain their practice”
If You’re Working Toward Becoming an Approved Supervisor
If you’re moving toward becoming an approved supervisor, it can be helpful to pause and take an honest look at where you are in the process.
Some questions I often encourage clinicians to reflect on include:
Where do I feel most confident — and where do I feel less certain — when it comes to clinical versus systems knowledge?
Have I had direct responsibility for another clinician’s work, and what did I learn from that experience?
Do I feel prepared to guide others in documentation, billing, and compliance, not just clinical care?
What areas would I want more support or consultation in before stepping into this role?
There isn’t one “right” path into supervision — but there is value in being intentional about how you get there.
Supervision is not just about supporting clinicians. It is about understanding how clinical work exists within systems—and holding responsibility for both. This is the level of awareness the 25-hour requirement is meant to build.
My Training and Approach to Supervision
My approach to supervision is grounded in both formal training and real-world experience across multiple practice settings.
This includes completion of structured supervision training programs focused on:
clinical supervision models
legal and ethical standards
documentation and compliance
risk management and liability
For example, I have completed formal supervision training, including a 15-hour clinical supervision course with law and ethics components , as well as advanced supervision coursework focused on systemic supervision models.
In addition to formal training, my experience includes supporting clinicians across:
agency and community mental health
integrated care settings
group practice
private practice development
This combination of training and applied experience shapes how I approach supervision — with attention to both clinical development and the systems that sustain practice. I also continue to engage in ongoing supervision training and development to maintain competency and stay aligned with evolving best practices in clinical supervision.
Support for Supervision of Supervision (Washington State)
If you’re working toward the 25-hour supervision of supervision requirement, I offer consultation designed to support that process in a thoughtful and practical way.
This work often includes:
Building a strong foundation in ethical and legal supervision
Developing confidence in documentation and oversight practices
Understanding systems like billing, credentialing, and compliance
Clarifying your approach and identity as a supervisor
The shift into supervision is not just a change in role— it’s a change in responsibility.
From your own clinical work… to holding responsibility for someone else’s.
And that requires more than clinical skill.
It requires systems awareness.
If you’re working toward becoming an approved supervisor, consider:
Do you feel confident in both clinical and systems knowledge?
Because supervision requires both.
Requirements vary by state and discipline, but the core expectation remains consistent: supervisors must be prepared to take responsibility for the clinical, ethical, and professional development of the supervisee.
References
Washington State Department of Health. (n.d.).
WAC 246-809-134: Approved supervisor.
https://app.leg.wa.gov/wac/default.aspx?cite=246-809-134
Washington State Department of Health. (n.d.).
WAC 246-809-334: Approved supervisor standards.
https://app.leg.wa.gov/wac/default.aspx?cite=246-809-334
Centers for Medicare & Medicaid Services (CMS). (n.d.).
National Plan and Provider Enumeration System (NPPES).
https://nppes.cms.hhs.gov
Centers for Medicare & Medicaid Services (CMS). (n.d.).
National Provider Identifier (NPI).
https://www.cms.gov/Regulations-and-Guidance/Administrative-Simplification/NationalProvIdentStand
Council for Affordable Quality Healthcare (CAQH). (n.d.).
CAQH ProView Provider Credentialing.
https://proview.caqh.org
Washington Health Care Authority. (n.d.).
ProviderOne Billing and Enrollment.
https://www.hca.wa.gov/billers-providers
OneHealthPort. (n.d.).
OneHealthPort Provider Portal.
https://www.onehealthport.com
Centers for Medicare & Medicaid Services (CMS). (n.d.).
PECOS (Provider Enrollment, Chain, and Ownership System).
https://pecos.cms.hhs.gov
Washington State Health Care Authority. (2019).
Integrated Managed Care SERI: NPI & Taxonomy Guidance.
SB Webb Counseling & Consulting PLLC | The Practice Library™
Clinical supervision and consultation with integrity, structure, and relational mentorship.
sbwebbcounselingconsulting.org
Stay Connected
I share articles, clinical reflections, and supervision resources periodically through The Practice Library.
If you’d like to stay connected, you’re welcome to follow along or join for updates.