

Let’s Graduate: Rethinking How We End Therapy
SB Webb Counseling & Consulting PLLC | The Practice Library™
sbwebbcounselingconsulting.org
Each time I facilitate my training, Let’s Graduate, I notice the same conversation begin to surface.
No matter the setting—medical clinics, community mental health, private practice, or supervision spaces—the same conversation emerges:
What do we actually call the end of therapy?
Do we call it graduation, case closure, termination, or discharge?
More importantly, what do those words reveal about how we understand care, transition, and our responsibility to ethical client care?
Language Is Not Neutral in Clinical Practice
In Washington State, our WACs refer to the “termination of services.” Personally, I don’t much care for the “T” word.
For example, under WAC 246-924-359, this language appears within a broader section on client welfare, which is important context. It emphasizes that when services end, clinicians are responsible for ensuring that clients are:
informed about their care and the nature of services provided
supported in accessing alternative services when needed
and not placed at risk due to disruption in treatment
It also reinforces that clients have a right to understand their treatment and exercise choice in their care, and that referrals must be made in the client’s best interest.
This language exists for a reason. It centers client welfare, continuity of care, and ethical accountability.
It also clarifies that clinicians have a responsibility to determine when treatment is no longer beneficial—or when it may even be harmful to continue.
From a regulatory standpoint, “termination” provides clarity and protection—for both the client and the provider.
But clinically?
The word termination often lands differently.
It can feel abrupt, final, and disconnected from the relational nature of therapy.
And yet, this is the language embedded in our documentation systems, our policies, and our training environments.
Over time, it doesn’t just shape how we write notes.
It shapes how we conceptualize the end of care.
Because of that, one of the core tensions I explore in this training—and more broadly within The Practice Library™—is this:
How do we uphold legal and ethical standards while still honoring the relational and human aspects of the work?
How do we meet regulatory expectations, document clearly and responsibly, and prevent abandonment—without reducing a meaningful therapeutic relationship to a single word that implies finality?
This question does not exist in isolation.
It connects directly to other areas of clinical practice, including how we:
conceptualize the therapeutic relationship as a primary mechanism of change
approach clinical documentation as both a legal and clinical narrative
and support clinicians in developing ethical, sustainable, and relationally grounded practice
Within The Practice Library™, this reflects a broader principle I return to often:
Clinical work requires integration—not separation—of relational depth, ethical responsibility, and structural accountability.
“The language we use in documentation shapes how we think about care—and how clients experience it.”
The Reality: Therapy Rarely Ends “Finally”
Therapy is rarely a one-time, linear episode of care.
Clients return, re-engage, and revisit therapy across different seasons of their lives—not because something has gone wrong, but because life continues to evolve.
Relationships shift.
Families expand or contract.
Health changes.
Loss occurs.
Roles and identities transform over time.
With each of these transitions, new layers of support may be needed.
From a clinical perspective, therapy is better understood as episodic, responsive, and contextual, rather than finite.
Clients may engage:
during periods of acute distress
for focused, goal-oriented work
or as part of ongoing wellness and self-reflection
Clinically, this often requires a shift away from a linear model of treatment toward a more flexible understanding of care across the lifespan.
This aligns with how we approach other areas of health.
We do not expect a single medical intervention to sustain lifelong well-being.
We return:
for preventative care
for maintenance
and when new concerns arise
Mental health care requires the same framework.
This shift matters.
Because when therapy is viewed as a one-time intervention, re-engagement can be misinterpreted as regression or failure.
When therapy is understood as episodic, re-engagement becomes what it often is:
a sign of insight, self-awareness, and appropriate use of support.
Endings Are Not Experienced the Same Way by Everyone
Termination, graduation, or transition is not only a clinical process.
It is also a cultural and relational experience.
In Let’s Graduate, I emphasize that clinicians must actively consider how endings are understood within the client’s broader context. This includes:
cultural meanings of endings and transitions
family and community norms around separation and continuity
experiences of loss, displacement, or historical trauma
expectations around ongoing connection versus closure
These factors shape not only how an ending is experienced, but how it is interpreted.
For some clients, the end of therapy may represent growth, accomplishment, and movement into a new phase of life.
For others, it may evoke grief, abandonment, or unresolved relational pain.
For many, it is both.
This is often where clinicians begin to recognize that these responses are not indicators of resistance or lack of progress—they are meaningful relational data.
This means that ending therapy is never just about clinical readiness.
It is about how that ending is experienced, understood, and integrated within the client’s cultural, relational, and historical context.
It is also important to recognize that many dominant models of psychotherapy are grounded in Western assumptions about closure—that it should be direct, explicit, and clearly defined.
This is not universal.
In some cultural contexts:
endings are not verbalized directly
continuity of relationship is expected
or relationships evolve rather than conclude
In others, structured acknowledgment and intentional closure may be deeply meaningful.
This requires clinicians to move beyond standardized approaches and instead engage in curiosity, humility, and collaboration.
A simple but clinically powerful question is:
“What would a respectful and meaningful ending look like for you?”
This approach is also consistent with ethical expectations around avoiding stereotyping and providing care that is responsive to the client’s lived experience.
Termination should not impose a cultural framework.
It should be co-created in a way that is culturally responsive, relationally meaningful, and experienced as safe by the client.
Re-Engagement Is Not Regression
One of the most important reframes in this work is this: returning to therapy is not a failure.
Clinicians are often working to challenge the assumption that re-engagement reflects a lack of progress. More often, it reflects something quite different.
It can represent:
self-awareness
intentional use of available resources
and adaptive coping across changing life circumstances
Clients may re-engage in therapy for a range of reasons, including:
significant life transitions (birth, loss, divorce, relocation)
environmental factors, such as seasonal patterns that impact mood and functioning
or emerging stressors that require additional support and integration
These are not signs that therapy “didn’t work.”
They are consistent with how people engage in care across the lifespan.
When therapy is understood as episodic rather than linear, re-engagement becomes clinically expected.
It reflects a client’s ability to:
recognize when additional support is needed
return to care proactively
and continue building on previous work
From this perspective, re-engagement is not regression.
It is continuity of care in action.
“Therapy is not something people complete—it is something they return to when life requires support.”
Ending Therapy Is Not About Permanence
Which brings us back to a core clinical shift stated earlier:
Ending therapy is not about permanence.
In practice, it is about transition, integration, and continued accessibility to care.
The goal is to support clinicians in moving away from a “closed case” mindset and toward a more longitudinal understanding of care.
From this perspective, the goal is not simply to end services, but to support a transition in which clients can:
integrate the work they have done
apply skills independently across environments
and maintain a clear understanding of how and when to re-engage if needed
Ending well means helping clients leave with:
skills they can use
insight they can carry
and a realistic expectation that support remains available as life evolves
This aligns with the broader understanding that therapy is not a one-time intervention, but a resource that can be accessed across the lifespan.
Ending therapy, then, is not about closing the door.
It is about equipping the client to move forward while knowing the door remains available.
Graduation as a Clinical Reframe
I intentionally use the word graduation.
In supervision and training, I often talk about how the language we choose shapes how we conceptualize the work—and how clients experience it. The term graduation reflects something different than “termination.”
It reflects growth, completion of a phase, readiness for increased independence, and the option to return if needed.
Therapy is not intended to create dependency.
It is intended to:
build skills
support insight
and increase capacity over time
From this perspective, the goal is not to maintain the therapeutic relationship indefinitely, but to support the client in functioning outside of it.
This is where the reframe becomes important.
Ending well is not about closing a chart.
It is about recognizing readiness—clinically, relationally, and contextually.
I often support and train clinicians in shifting from a completion-based mindset to a readiness-based framework.
Graduation is not simply the point at which goals have been met on paper.
It is the point at which the client is prepared to sustain their progress beyond the structure of therapy.
“Graduation is not about completion. It is about sustainability.”
Graduation Begins at Intake
One of the most important clinical shifts is this:
Graduation is not something we decide at the end of therapy. It is something we begin preparing for at the beginning.
From the first session, clients benefit from understanding that therapy is structured, goal-oriented, and intended to support increasing independence over time.
This begins at intake.
Within The Practice Library™, I often refer to this as establishing the golden thread—the clinical connection between:
the client’s presenting concerns
the treatment plan
the work done in session
and the eventual transition out of care
When this thread is clear, therapy has direction.
When it is not, therapy can become reactive and fragmented.
This early work includes:
discussing the purpose and scope of treatment
establishing initial, measurable goals
and setting expectations that therapy is not indefinite, but responsive to progress and need
This is also consistent with ethical expectations that clients are informed about the nature and purpose of treatment and have a clear understanding of their care.
Without this foundation, termination can feel abrupt, unclear, or even destabilizing.
With it, graduation becomes expected, collaborative, and clinically meaningful.
Treatment planning plays a critical role in maintaining this trajectory.
Clearly defined goals provide both direction and a finish line, even as those goals evolve over time.
In consultation, clinicians often begin to recognize that without a defined trajectory, therapy can shift into a pattern of responding only to immediate concerns—what might show up session to session—without sustained movement toward longer-term outcomes.
Establishing and revisiting goals helps anchor the work.
It ensures that therapy remains purposeful, that progress is tracked over time, and that graduation is integrated throughout the process—not introduced at the end.
“If case closure is a surprise, something in the process was missed.”
But What Does “Ready” Actually Mean?
Readiness Is Not One-Dimensional
Clinical readiness is not a single decision point.
It requires consideration of multiple layers.
This process often requires slowing down and asking more precise questions:
Is the client ready to end therapy altogether?
Or are they ready to complete this phase of work?
Is this a graduation, a transition, or a transfer?
Clients may:
meet initial treatment goals
complete a specific modality
or reach stability in one domain
while still benefiting from continued or different forms of care.
Ending one phase of therapy does not necessarily mean the work is complete.
It may mean:
The work is evolving.
Differentiating Graduation, Transition, and Transfer
A critical clinical distinction is between:
Graduation: The client has met their goals, is stable, and is ready to transition out of care
Transition: The client has completed a phase or modality and is moving into a different type of work
Transfer: The client requires a different provider or level of care to meet their needs
This distinction helps prevent:
premature termination
missed opportunities for continued growth
and confusion for both client and clinician
Applying This Across Modalities
This becomes especially important when we consider different treatment approaches.
For example:
A client may complete a CBT-focused episode of care and demonstrate improved coping skills, but still benefit from deeper relational or trauma-focused work.
A client may complete EMDR processing for a specific target but continue to experience broader attachment or identity-related concerns.
A client may complete a DBT skills group and show improved regulation, while still needing support integrating those skills into relationships or life transitions.
In each of these cases, the client may be:
ready to transition, but not necessarily ready to graduate from therapy entirely.
Readiness Requires Clinical Judgment
This is where clinical clarity becomes essential.
In both training and clinical supervision, I emphasize that graduation should not be based on instinct, convenience, or external pressures.
Decisions about ending care require a thoughtful, structured assessment of readiness.
Graduation should be grounded in clearly identifiable indicators, including:
Treatment goals are largely met
Improved functioning across environments
Stability in symptoms and behaviors over time
External supports are available and accessible
Skills are generalized and used outside of sessions
Crisis risk is stable or meaningfully reduced
The client expresses readiness to transition
These indicators help ensure that the decision to end therapy is not based solely on progress observed within sessions, but on the client’s ability to sustain that progress in their daily life.
A Shift in Clinical Thinking
This reflects a shift away from a completion-based model to a sustainability-based model.
Rather than asking:
“Are we done?”
The more clinically useful question becomes:
“Is this sustainable outside of therapy, across environments, and over time?”
Clients may demonstrate:
insight
emotional regulation
or behavioral change
within the structure of therapy.
However, graduation requires confidence that these gains are:
transferable
maintained
and supported beyond the therapeutic relationship
When this level of readiness is present, graduation becomes a clinically appropriate transition—not simply the conclusion of a treatment plan, but the next phase of independent functioning.
Clinical readiness is not a single decision—it is a multidimensional assessment that can be organized into key domains.

A clinical framework outlining key domains of readiness for graduation from therapy, including stability, skill use, external supports, and long-term sustainability. This framework is part of The Practice Library™, a collection of clinical tools supporting ethical and sustainable therapy practice.
In addition to conceptual understanding, clinicians benefit from clearly defined indicators that support ethical and clinically appropriate graduation decisions.
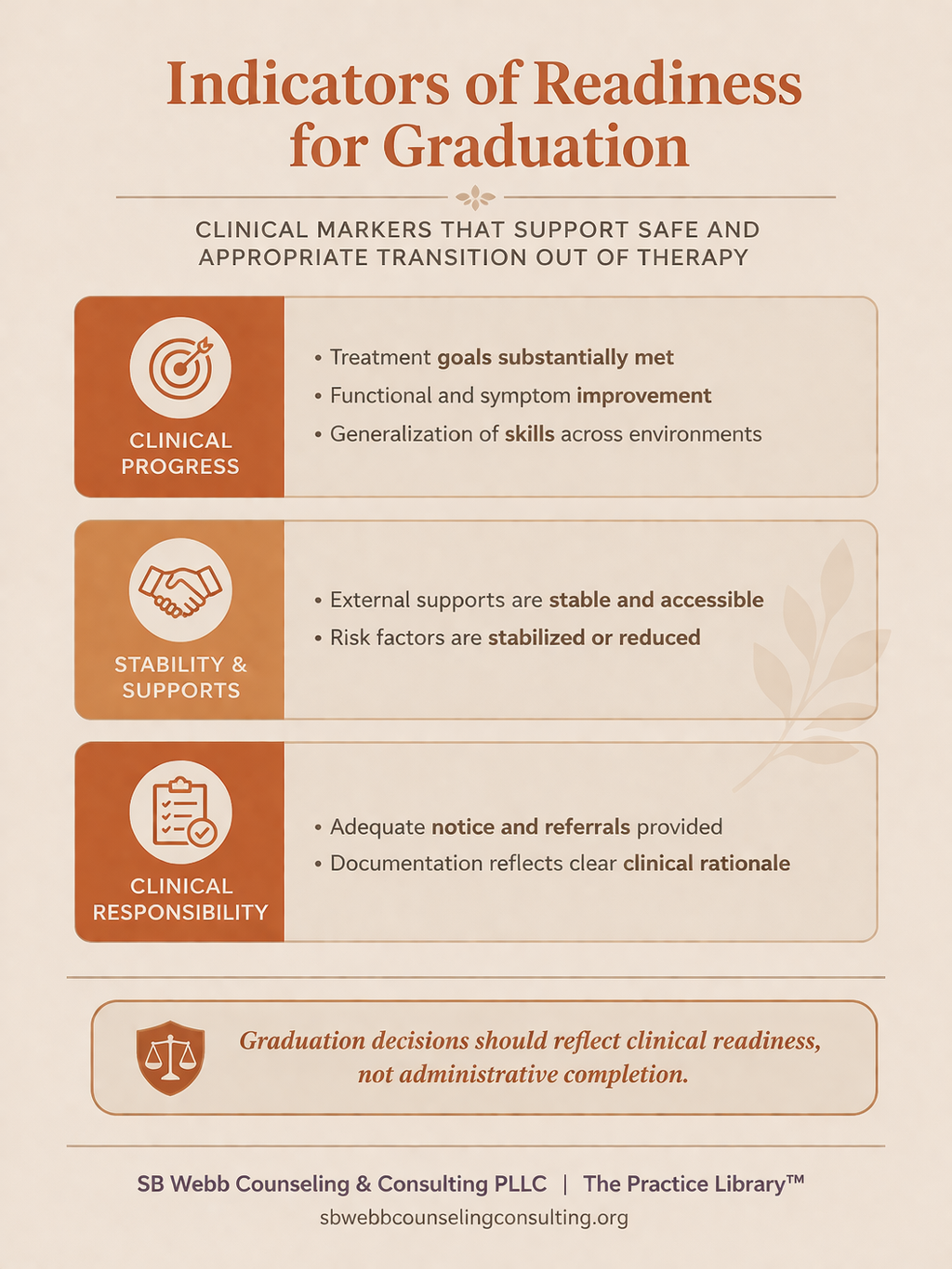
A structured checklist of clinical indicators for therapy graduation, including goal completion, functional improvement, risk stabilization, and documentation requirements. This framework is part of The Practice Library™, a collection of clinical tools supporting ethical and sustainable therapy practice.
Graduation Requires a Conversation—Not a Decision
Even when a client appears clinically ready, graduation should not be treated as a singular decision point.
It is a process that is developed, revisited, and reinforced over time.
In both training and clinical supervision, I emphasize that conversations about ending therapy should not begin at the final phase of treatment. They should be introduced early and revisited consistently throughout the course of care.
When this is done well, graduation is not experienced as abrupt or unexpected—it is understood as part of the therapeutic process.
What I often see in practice is that clinicians are making decisions about readiness in isolation, without enough structure or support.
This is where supervision and consultation become essential.
Within supervision, these conversations allow clinicians to:
assess readiness with greater clinical clarity
differentiate between graduation, transition, and transfer
and identify whether progress is sustainable beyond the therapy setting
Supervision provides a space to slow the process down, examine assumptions, and ensure that decisions are grounded in clinical reasoning—not urgency, discomfort with endings, or external pressures.
This also connects to the broader clinical ecosystem surrounding the client.
Graduation is not simply about what happens within the therapy room.
It requires consideration of:
the client’s support systems
their environment and ongoing stressors
access to additional resources
and the continuity of care if re-engagement becomes necessary
When clinicians are supported in thinking systemically, graduation becomes more than a decision—it becomes a coordinated transition within a larger network of care.
Within The Practice Library™, this is where supervision, consultation, documentation, and clinical decision-making intersect.
Graduation is not a standalone event.
It is the outcome of:
intentional treatment planning
ongoing assessment
structured dialogue
and supported clinical judgment
When these elements are in place, graduation becomes:
collaborative
predictable
and clinically meaningful
Rather than something that happens at the end, it becomes something that is built into the work from the beginning and supported throughout the entire course of care.
Embedding Graduation into the Treatment Process
One of the most effective ways to support this is through intentional treatment planning.
Treatment plans should not only outline clinical goals, but also establish a clear direction toward completion.
Within The Practice Library™, this is part of maintaining the golden thread—ensuring that what is identified at intake continues to guide the work across sessions and toward an eventual transition.
Without this structure, therapy can become reactive—shifting from one immediate concern to the next without a defined trajectory.
Clients frequently present with immediate or situational stressors that require attention. While these concerns are valid, when sessions become consistently driven by short-term crises, the broader direction of treatment can begin to drift.
Over time, this can result in:
stalled progress
unclear treatment goals
and difficulty determining readiness for graduation
A structured approach allows clinicians to remain responsive while maintaining direction.
This includes:
acknowledging and addressing present concerns
while intentionally returning to the broader treatment goals
This balance ensures that therapy remains both responsive and purposeful, rather than reactive.
Regularly revisiting the treatment plan helps to:
reinforce the purpose of therapy
track progress over time
and maintain alignment with intended outcomes
It also supports ongoing assessment of readiness, rather than leaving that determination to the end of treatment.
When appropriate, clinicians may include graduation or transition goals within the treatment plan itself.
This makes the trajectory of care explicit, reinforces expectations of progress and independence, and reduces the likelihood that ending therapy will feel abrupt or unanticipated.
Ongoing Assessment Through Structured Dialogue
As treatment progresses, clinicians should be engaging in ongoing conversations about readiness, rather than waiting until goals are nearly complete.
Some of the most clinically useful questions include:
What changes have you noticed since starting therapy?
How are you applying skills outside of session?
What concerns do you have about ending therapy?
What support systems will help you after graduation?
What situations might challenge your progress?
What is your plan if symptoms return?
Ongoing assessment of readiness is best supported through structured clinical dialogue, not a single end-of-treatment conversation.
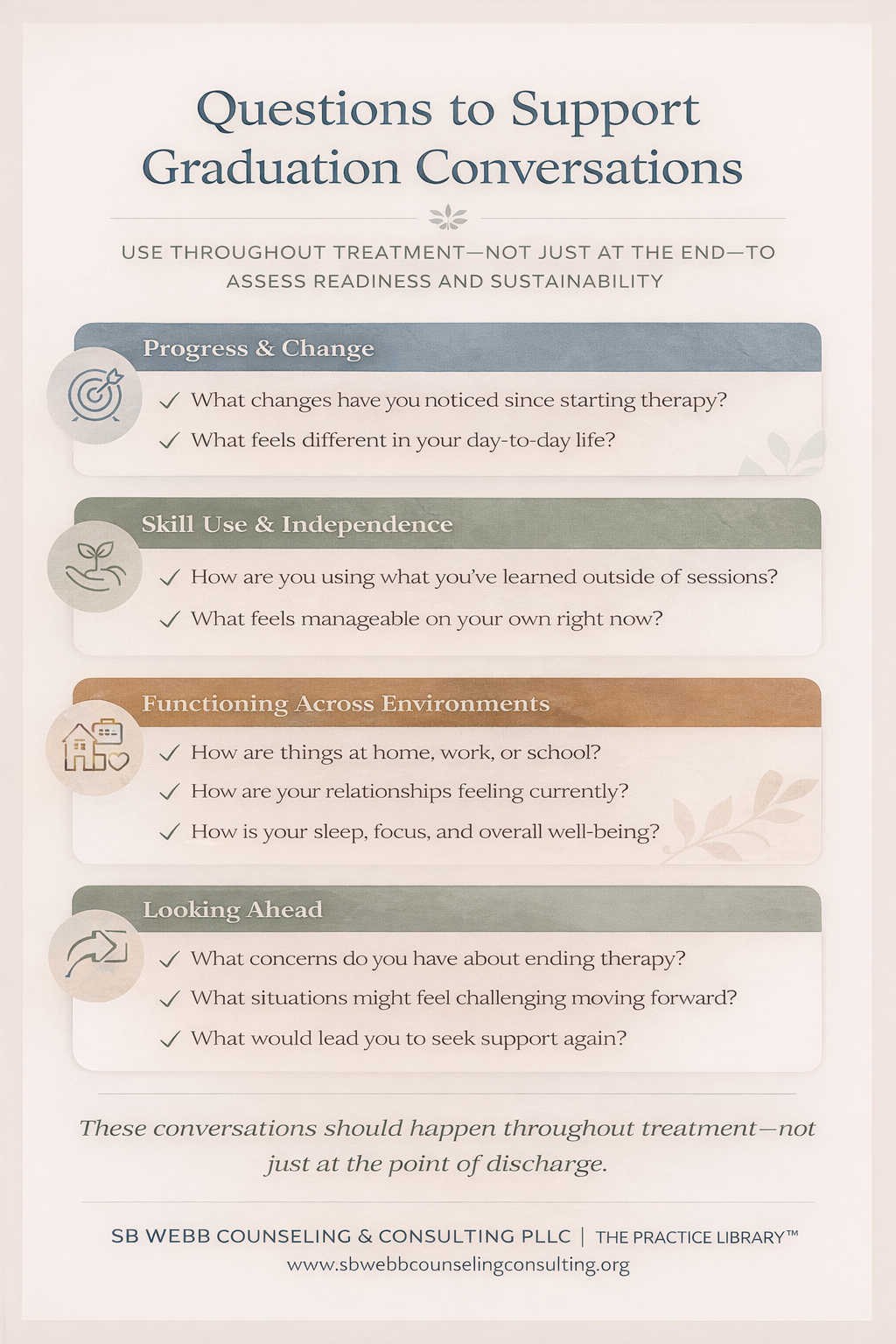
A set of clinical questions used throughout therapy to assess progress, skill use, functioning across environments, and readiness for transition out of care. This framework is part of The Practice Library™, a collection of clinical tools supporting ethical and sustainable therapy practice.
These questions are not reserved for the final phase of treatment.
They should be introduced and revisited throughout care to:
reinforce skill generalization
support future-oriented thinking
and normalize the eventual transition out of therapy
In addition to structured dialogue, clinicians may also incorporate brief assessments and outcome measures to support clinical decision-making.
This might include:
symptom rating scales (e.g., PHQ-9, GAD-7)
functioning assessments
or individualized measures tied to treatment goals
Supervision can support the integration of both clinical dialogue and measurable indicators.
When used thoughtfully, brief assessments can:
provide objective data on symptom change over time
support conversations about readiness and progress
strengthen clinical documentation
and reduce reliance on subjective impressions alone
This combination helps ensure that readiness is not determined by a single conversation or moment in treatment, but through ongoing, multidimensional assessment.
A Shift in Clinical Thinking
This reflects a broader shift in clinical thinking.
Rather than asking, “Are we done?”
The more clinically useful question becomes:
“Is this client prepared to sustain their progress outside of therapy—across environments and over time?”
This shift matters.
Because progress within the structure of therapy does not always translate to sustained functioning outside of it.
Graduation requires confidence that gains are:
transferable
maintained
and supported beyond the therapeutic relationship
The Role of the Ecosystem (Not Just Symptoms)
One of the most common clinical pitfalls is focusing primarily on symptom reduction.
But people do not live in symptoms.
They live in systems.
Using tools such as an eco-map, clinicians can more fully assess the context in which progress is occurring. This includes examining:
relational dynamics
environmental stressors
reciprocity within relationships
and stability across key life domains
Because sometimes the symptoms are improving—
but the system is not yet stable.
A client may demonstrate reduced anxiety or improved mood in session, while still navigating:
unstable relationships
environmental stressors
or limited external support
In these cases, graduation may be clinically premature—not because progress has not occurred, but because it has not yet been sufficiently supported within the client’s environment.
Graduation should reflect whole-person readiness, not just progress on paper.
This is also where cultural responsiveness becomes essential.
The client’s ecosystem includes not only relationships and environment, but also cultural context—which shapes how connection, separation, and transition are understood.
Rather than applying a standardized approach to termination, clinicians should adapt the process in ways that align with the client’s cultural and relational world.
This may include:
modifying closure activities
incorporating family or community supports
or adjusting expectations around ongoing connection
The goal is not to apply a uniform termination process.
It is to create one that is culturally responsive, relationally meaningful, and experienced as safe by the client.
Transfers Are Not Neutral
Another key teaching point is this:
Transfers are not just administrative—they are relational events.
Clinically, it is important to recognize that a transfer can carry many of the same emotional and clinical implications as closure, and therefore should be treated as a parallel process.
Clients may experience:
loss of relationship
uncertainty about what comes next
fear of starting over
or concern about whether they will be understood
These responses are not uncommon. They reflect the reality that a therapeutic relationship has meaning.
Because of this, transfers require more than coordination—they require clinical intention.
They involve:
preparation
emotional processing
and continuity planning
A transfer done poorly can feel like abandonment.
A transfer done well can feel like a supported and structured transition.
From a clinical and ethical perspective, transfers require many of the same considerations as termination, including:
adequate notice
continuity of care
informed consent
and clear, coordinated communication
This includes communication not only with the client, but—when appropriate—between clinicians to support continuity and reduce fragmentation of care.
Both the outgoing and receiving clinician play a role in shaping the client’s experience.
When handled well, a transfer models:
predictability
safety
and relational continuity
It reinforces that care is not being withdrawn—it is being continued in a different form.
When handled poorly, transfers can reinforce existing narratives of:
abandonment
instability
or mistrust
Particularly for clients with histories of relational disruption, these experiences can carry significant weight.
As clinicians, we reframe transfers as:
a guided transition—not a withdrawal of care.
“A transfer is not leaving a client—it is guiding them into their next phase of care.”
Preventing Abandonment Is an Ethical Imperative
One of the most critical aspects of ending care is ensuring that we are not unintentionally abandoning clients.
This is often an area where clinicians experience the most uncertainty—particularly when balancing ethical responsibility with clinical judgment about readiness.
Preventing abandonment requires intentional planning throughout the course of care, not just at the point of discharge.
This includes:
discussing the possibility of termination early and revisiting it over time
providing adequate notice when services are ending
documenting efforts to contact and engage clients
offering referrals and alternative resources when appropriate
ensuring continuity of care, particularly for higher-risk clients
and clearly documenting the clinical rationale for ending services
These are not simply best practices.
They are ethical responsibilities that align with broader expectations around client welfare, continuity of care, and appropriate transition planning.
It is equally important to clarify what abandonment is—and what it is not.
Abandonment occurs when a clinician ends services without ensuring that the client’s ongoing treatment needs are appropriately supported, creating a foreseeable risk of harm.
It is not abandonment when:
a client disengages from treatment
declines referrals
or chooses to end services independently
It is also not abandonment when services are ended:
with appropriate notice
with clear clinical rationale
and with transition planning in place
This distinction is essential.
In both clinical practice and supervision, fear of abandonment can sometimes lead clinicians to avoid appropriate termination, extend care beyond clinical necessity, or hesitate to make transitions that would better serve the client.
Clear understanding allows clinicians to act ethically while still exercising sound clinical judgment.
The Often-Missed Step: Therapist Self-Reflection
One of the most powerful—and often underutilized—parts of this process is clinician reflection.
This is a place where slowing down is essential. Supervision models this process, as relationships evolve, transition, and come to a close over time.
Before ending, we should be asking ourselves:
How do I feel about this client’s graduation?
Is there anything left unsaid therapeutically?
What growth have I observed in this client over time?
How have I contributed to their progress?
Am I avoiding any conversations about ending?
How can I model a healthy, intentional goodbye?
These questions are not just reflective—they are clinical.
They help us identify:
avoidance
attachment dynamics
unresolved therapeutic material
and opportunities for meaningful closure
Because endings are not only clinical.
They are relational—for both people in the room.
How a clinician navigates the ending of therapy can model:
emotional presence
clear communication
and the ability to engage in a relationship that can both form and conclude safely
When we approach endings with this level of intentionality, we are not just completing treatment.
We are reinforcing one of the most important therapeutic experiences a client can have:
a relationship that ends with care, clarity, and respect.
Supporting Clients in Preparing for Graduation
Clients benefit from structure as they prepare to transition out of therapy.
In supervision, I often emphasize that graduation is not simply something we assess—it is something we actively prepare clients for over time.
This preparation helps clients consolidate their progress and approach the transition with clarity and confidence.
This may include:
reviewing progress and goals achieved
identifying coping strategies that are effective and sustainable
developing a long-term wellness or maintenance plan
updating relapse prevention or safety plans as needed
identifying support systems and resources
and understanding how to reconnect with services if needed
Preparing for graduation is an active process that includes reflection, planning, and supporting continuity of care beyond therapy.

A step-by-step clinical process for therapy graduation, including timeline development, celebrating progress, identifying warning signs, and planning for re-engagement or referrals. This framework is part of The Practice Library™, a collection of clinical tools supporting ethical and sustainable therapy practice.
This process reinforces a broader clinical goal:
not just symptom improvement, but ongoing self-management and access to support.
It also helps normalize that future support may be needed.
Rather than framing therapy as something that ends completely, this approach reinforces that clients can return to care intentionally, as new needs arise.
This reinforces an important message:
You are not being discharged. You are being prepared.
The Clinical Importance of Celebration
There is something else I have noticed in this work.
As adults, we rarely pause to acknowledge growth.
We move quickly from one demand to the next, often without recognizing the effort it took to get there.
Therapy offers a different opportunity.
It creates space to:
name change
acknowledge effort
and sit with success
In supervision, I often remind clinicians that this is not just a “nice moment” at the end of treatment.
It is clinically meaningful.
Helping clients recognize their progress supports:
integration of the work
reinforcement of self-efficacy
and a more accurate internal narrative of growth
For some clients, this may feel unfamiliar or even uncomfortable.
Celebration can bring up:
vulnerability
difficulty receiving acknowledgment
or beliefs about worthiness
That, too, becomes part of the work.
And for some clients?
Simply being able to sit with their own progress—to recognize it, name it, and allow it to exist—
is powerful.
Ending Well Is a Clinical Skill
What I continue to learn through facilitating Let’s Graduate is this:
Ending therapy well is not a form, a checkbox, or a final note.
It is a clinical, ethical, and relational process.
And how we do it matters.
It is important that, as clinicians, we recognize that endings are not separate from treatment.
They are part of it.
Ending well requires:
structure
preparation
collaboration
and clinical intentionality
It requires us to:
assess readiness thoughtfully
engage in ongoing dialogue
consider the client’s ecosystem and cultural context
support transition and continuity of care
and approach the ending as a meaningful relational experience
This is not something we improvise at the end of treatment.
It is something we build toward throughout the entire course of care.
When done well, the ending of therapy becomes more than a conclusion.
It becomes an opportunity to model:
clarity
respect
emotional presence
and a relationship that can both begin and end safely
This is the work we are responsible for as clinicians.
This framework is not developed in isolation.
It reflects an integration of relational, behavioral, narrative, and ethical approaches to understanding how therapy ends.
“Ending well is not the end of therapy—it is part of the treatment.”
Clinical Foundations
Tsai, M., Gustafsson, T., Kanter, J., Plummer Loudon, M., & Kohlenberg, R. J. (2017). Saying good goodbyes to your clients: A Functional Analytic Psychotherapy (FAP) perspective. Psychotherapy, 54(1), 22–28: This article provides a foundational relational framework for understanding termination as an opportunity to evoke vulnerability, reinforce growth, and support meaningful interpersonal closure. It emphasizes that endings in therapy can serve as a powerful extension of the therapeutic process itself.
Barnett, J., & Coffman, C. (2015).Termination and abandonment: A proactive approach to ethical practice: Offers clear guidance on ethical termination, including abandonment prevention, documentation standards, and continuity of care. This work reinforces the importance of aligning relational practice with legal and ethical obligations.
Leahy, R. (2017). CBT termination strategies: Preventing relapse and consolidating skills: Offers structured, skills-based approaches to termination, including relapse prevention and consolidation of therapeutic gains. Complements relational approaches by supporting long-term sustainability.
White, M. (2007). Narrative therapy: Maps of practice — Re-authoring conversations: Provides narrative frameworks that support clients in integrating their therapy experience into their broader life story, including meaning-making practices relevant to termination and transition.
SB Webb Counseling & Consulting PLLC | The Practice Library™
Clinical supervision and consultation with integrity, structure, and relational mentorship.
sbwebbcounselingconsulting.org
For Clinicians
If you are navigating these questions in your clinical work, you are not alone.
These are the same conversations I support in: