

From Diagnosis to Understanding: What the DSM-5 -TR Doesn’t Teach You About Clinical Thinking
SB Webb Counseling & Consulting PLLC | The Practice Library™
sbwebbcounselingconsulting.org
For many clinicians in training, learning the DSM-5-TR is framed as a foundational milestone. It offers structure, clarity, and a shared professional language. It helps answer an early and pressing question:
“What is going on with this person?”
But over time, a more complex question begins to emerge:
“How do I actually understand what I’m seeing?”
Because while the DSM-5-TR provides a framework for classification, it does not fully teach how to think clinically, how to weigh context, hold ambiguity, or integrate multiple layers of human experience.
That part develops elsewhere and often, without being explicitly named or taught.
The Illusion of Certainty
“Diagnosis is not about certainty—it is about working hypotheses.”
Early in training, diagnosis can feel like a process of finding the “right answer.” Criteria are reviewed, checklists are considered, and clinicians are often reinforced for accuracy and precision.
But clinical work rarely presents in clean, discrete categories.
Symptoms overlap. Context shifts. Presentations evolve. And individuals often hold multiple, interacting experiences that do not fit neatly into a single diagnostic frame.
The expectation of getting it “exactly right” can create pressure for clinicians to arrive at conclusions prematurely, sometimes at the expense of deeper understanding. This pressure is particularly strong for early-career clinicians, where uncertainty can feel like a personal failure rather than a normal part of development (see The First Five Years of Clinical Practice: Why Therapists Burn Out Early).
Over time, many clinicians begin to recognize that diagnosis is not about certainty - it is about working hypotheses, shaped and reshaped through ongoing assessment.
What the DSM-5-TR Is and What It Is Not
The DSM-5-TR serves several essential functions:
A standardized system for identifying mental health conditions
A shared language across providers and disciplines
A foundation for treatment planning and communication
In practice, clinicians also translate diagnoses into ICD-10 codes (World Health Organization, 2019), situating diagnosis within healthcare systems, documentation requirements, and reimbursement structures.
At the same time, diagnosis is guided by professional responsibility. Across disciplines, codes of ethics (NASW, ACA, AAMFT, APA) emphasize that diagnosis must be applied with competence, cultural awareness, and care.
Taken together, diagnosis exists at the intersection of:
Clinical frameworks (DSM-5-TR)
Administrative systems (ICD-10)
Ethical standards (professional codes of ethics)
And yet, even within these structures, something is still missing.
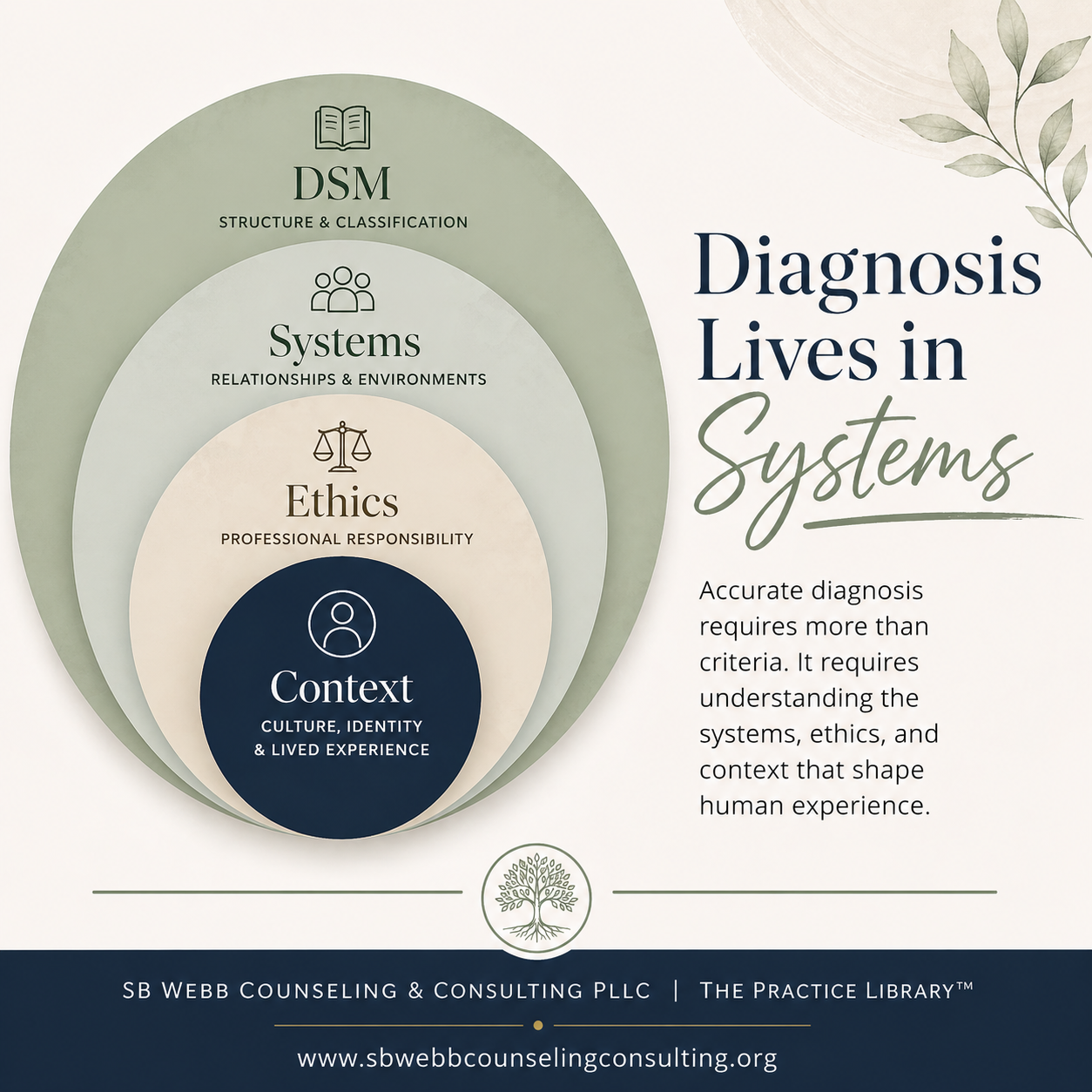
Diagnosis Lives in Context
Long before modern diagnostic manuals, social work emphasized the importance of context. Mary Richmond’s early work on social diagnosis framed assessment as a process of understanding individuals within their environments - not separate from them.
This perspective continues through the person-in-environment lens, which recognizes that symptoms cannot be fully understood without considering relationships, social conditions, and lived experience.
Ecological systems theory (Bronfenbrenner) further expands this view, highlighting how individuals are shaped by multiple, interacting systems:
Family
Community
Institutions
Broader societal structures
Taken together, these frameworks move clinical work away from reductionist classification and toward integrated understanding - where diagnosis becomes one component of a broader formulation rather than the endpoint.
Relational and Systemic Understanding
Clinical work does not happen in isolation, and neither does distress.
Family systems theory reminds us that individuals exist within relational networks where patterns, roles, and dynamics influence both symptoms and healing. What appears as an individual diagnosis may, in reality, reflect relational stress, intergenerational patterns, or systemic strain.
Similarly, trauma-informed care shifts how symptoms are interpreted. Rather than asking “What is wrong with this person?” clinicians are invited to consider:
“What has happened and how has this person adapted?”
This reframing recognizes that many symptoms represent adaptive responses to adversity, not simply disorders to be categorized.
“Diagnosis is not a label. It is a formulation shaped by context, systems, and lived experience”
Culture, Equity, and Whole Person Health
Modern clinical practice increasingly recognizes that diagnosis cannot be separated from culture, identity, and systems of power.
Frameworks grounded in diversity, equity, and inclusion (DEI) highlight the importance of:
Cultural context
Structural inequities
Bias in diagnostic systems
Without attention to cultural context and systemic inequities, diagnosis risks reinforcing existing disparities, particularly when diagnostic frameworks are applied without consideration of bias, access, and lived experience.
At the same time, whole person health approaches emphasize that mental health is interconnected with:
Physical health
Social conditions
Environmental stressors
Access to care
This broader lens challenges reductionist thinking and supports a more integrated understanding of well-being.
Co-Occurring Conditions and Clinical Complexity
In real-world practice, individuals rarely present with a single, clearly defined condition.
Instead, clinicians often encounter co-occurring concerns, including:
Mental health conditions
Substance use
Medical conditions
Psychosocial stressors
These layers interact in ways that evolve over time, reinforcing that diagnosis is not a fixed conclusion—it is a working formulation. In this, Diagnosis is best understood not as a static label, but as a clinical argument grounded in evidence, presentation, and functional impairment.
Assessment as an Ongoing Process
Clinical assessment is not a one-time event. It is a process that deepens with:
Time
Relationship
Additional information
Shifts in context
Tools such as eco-maps can support this process by visually mapping relationships, supports, and stressors within a person’s environment. These tools help move beyond diagnostic criteria alone and toward a more comprehensive understanding of lived experience.
As clinicians grow, diagnosis becomes less about accuracy in a single moment and more about refining understanding over time.
Diagnosis, Identity, and Meaning
Diagnosis does not exist in a vacuum.
Erving Goffman’s work on stigma reminds us that labels can shape not only how individuals are perceived—but how they come to understand themselves.
Because of this, diagnosis carries weight. It has implications for:
Identity
Access to care
Social perception
Internalized meaning
This reinforces the importance of using diagnosis thoughtfully, ethically, and with awareness of its broader impact.
From Classification to Clinical Thinking
Early in training, clinicians often focus on “getting the diagnosis right.”
Over time, the focus shifts. This shift becomes visible in documentation, where clinical thinking is translated into defensible, structured reasoning (see Documentation Is Clinical Thinking Made Visible).
Diagnosis becomes less about selecting the correct label and more about:
Understanding patterns
Integrating context
Remaining open to change
Holding complexity without rushing to certainty
This is where clinical thinking develops—not through memorization, but through experience, supervision, and reflection.
What This Means for Clinicians in Training
For clinicians in training, this stage can feel disorienting.
You may be taught to focus on criteria, accuracy, and getting the diagnosis “right.” At the same time, you may begin to notice that real clinical presentations are more complex than what is outlined in a manual.
It is not uncommon to feel uncertain, to question your judgment, or to wonder whether you are missing something.
This is not a sign that you are doing something wrong—it is a sign that you are beginning to think clinically.
Clinical thinking develops over time. It is shaped through supervision, experience, and reflection. It involves learning how to hold multiple possibilities, integrate context, and remain open to change.
Diagnosis becomes less about arriving at a fixed answer and more about developing a thoughtful, evolving understanding.
“Over time, clinicians begin to shift from certainty toward curiosity—and it is within that shift that clinical thinking develops.”
Closing: An Evolving Understanding
If diagnosis is treated as static, it risks oversimplifying complex human experiences.
If understood as ongoing, it becomes something else entirely:
A tool for curiosity
A process of refinement
A way of integrating multiple layers of understanding
The DSM-5-TR provides structure.
But structure alone is not sufficient.
Clinical thinking develops in context—through supervision, systems, relationships, and lived experience.
And over time, diagnosis becomes less about identifying what is “wrong” and more about understanding what is true, complex, and still unfolding.
That shift—from certainty to curiosity, from classification to formulation—is what ultimately allows clinicians not only to diagnose, but to truly understand.
This is the shift that defines the transition from student to clinician.
As you continue your training, consider:
Are you trying to get the diagnosis exactly right—or are you learning how to understand what you’re seeing over time?
References
American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR).
World Health Organization. (2019). International Classification of Diseases, 10th Revision (ICD-10).
National Association of Social Workers. (2021). Code of Ethics.
American Counseling Association. (2014). ACA Code of Ethics.
American Association for Marriage and Family Therapy. (2015). AAMFT Code of Ethics.
American Psychological Association. (2017). Ethical Principles of Psychologists and Code of Conduct.
Bronfenbrenner, U. (1979). The Ecology of Human Development.
Goffman, E. (1959). The Presentation of Self in Everyday Life.
Richmond, M. (1917). Social Diagnosis.
SB Webb Counseling & Consulting PLLC | The Practice Library™
Clinical supervision and consultation with integrity, structure, and relational mentorship.
sbwebbcounselingconsulting.org
If you’re seeking clinical supervision or consultation grounded in clinical thinking, structured reflection, and systems-informed practice, you can learn more below—and explore how this work develops over time.
Stay Connected
I share articles, clinical reflections, and supervision resources through The Practice Library™